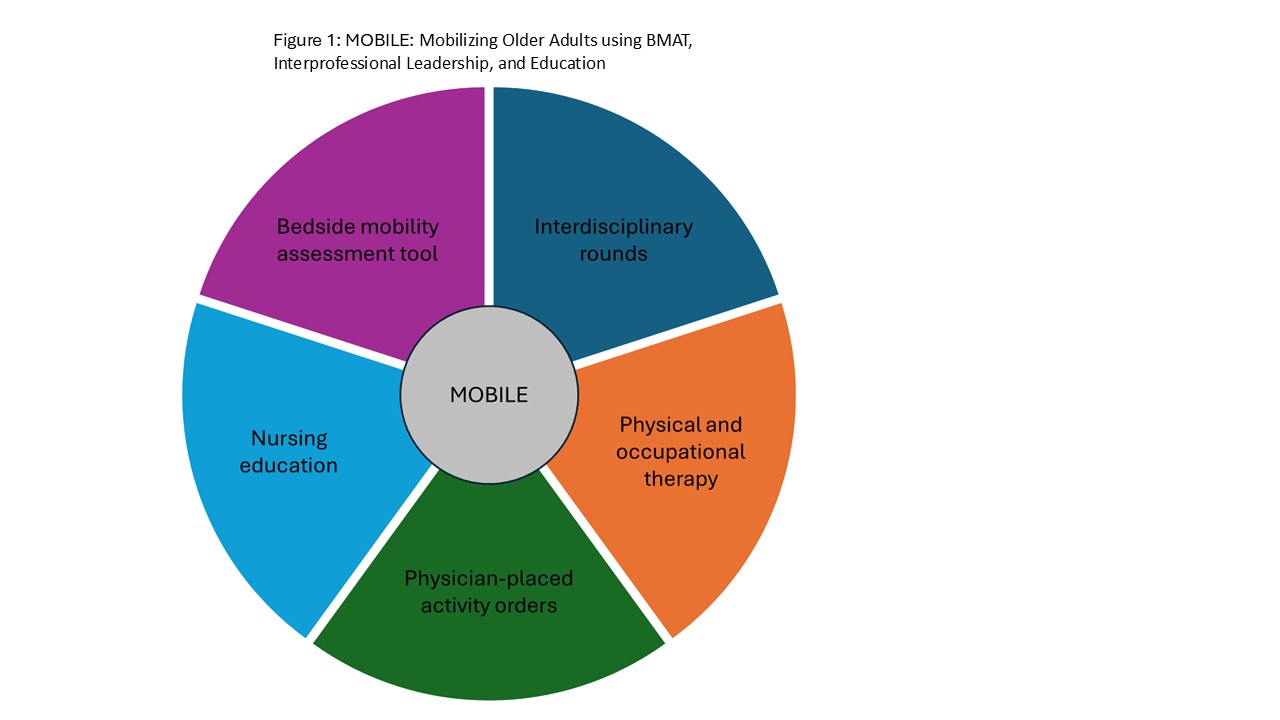
Background: Acute illness contributes to deconditioning of hospitalized older adults, significantly impacting their short- and long-term outcomes. The Banner Mobility Assessment Tool (BMAT) was developed to guide nurses in assessing mobility when promoting physical activity for their patients. We implemented a quality improvement initiative, “Mobilizing Older Adults using BMAT, Interprofessional Leadership, and Education (MOBILE)”, which incorporates BMAT as the mobility assessment tool, and we assessed its impact on preventing functional decline in hospitalized older adults.
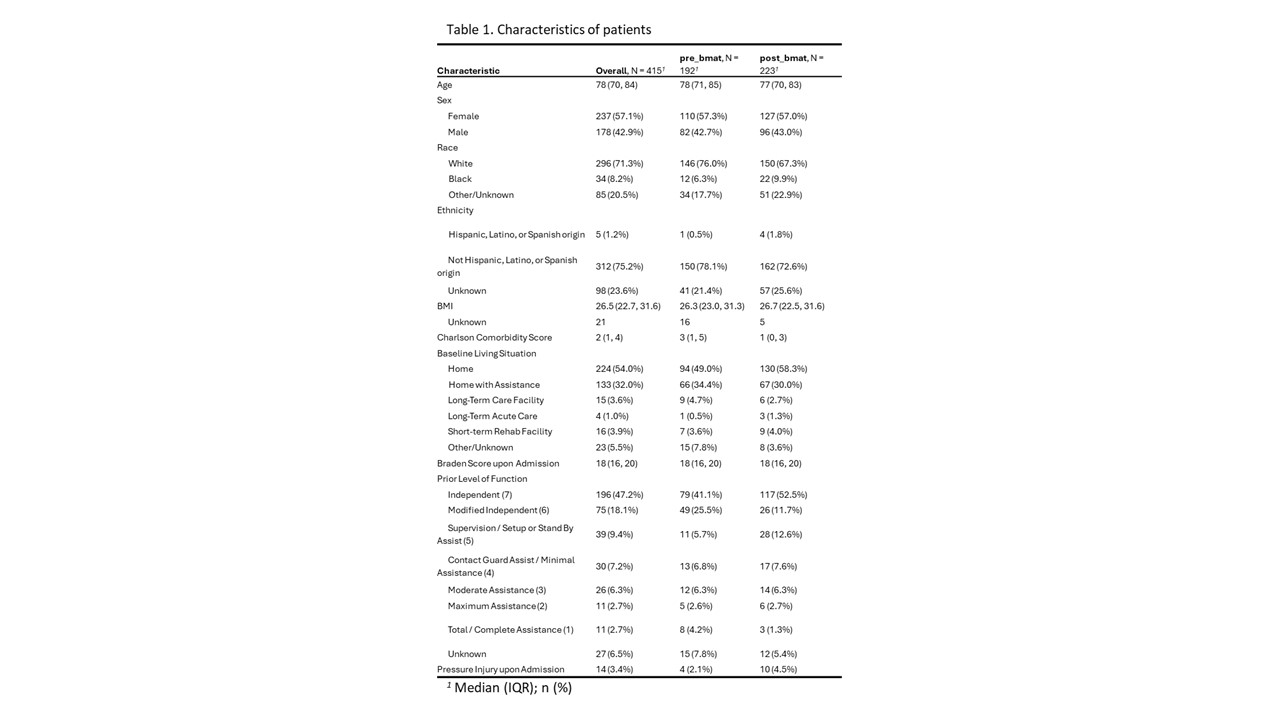
Methods: We implemented MOBILE at a 13-bed ACE unit in a 537-bed community teaching hospital in October 2022. Implementation strategies included education, training, and integration into existing workflows (Figure 1). We collected data on all patients age ≥65 years who were admitted to the ACE unit during the pre-implementation (July-September 2022) and post-implementation (December 2022-Feburary 2023) period. Patients who expired or discharged to hospice were excluded. Data included patient characteristics and prior level of function (Table 1). Primary outcome was functional decline. Other clinical outcomes included length of stay (LOS), falls, and new or worsening pressure injuries. Statistical analyses were conducted using Wilcoxon rank sum, Fisher’s exact, and Pearson’s Chi-squared tests.
Results: Of 415 eligible patients included in this analysis, 192 (46.3%) were admitted prior to and 223 (53.7%) after MOBILE implementation. The MOBILE intervention was associated with higher rates of patients having at least one BMAT assessment completed (72.6% vs 30.7% at baseline, p<.001) and higher rates of activity order placement (57.4% vs 32.8% at baseline, p<.001). The frequency of functional decline was lower post-MOBILE implementation compared to pre-MOBILE implementation (24.2% vs 35.0%, respectively, p=.02). However, after adjusting for age, sex, body mass index, Charlson comorbidity score and Braden score, we did not find any association between functional decline and MOBILE (adjusted Odds Ratio, 0.65; 95% confidence interval, 0.39-1.07). The post- vs pre-MOBILE median LOS (3 days [IQR, 2-5 days] vs 3 [IQR, 2-5 days], p=.65), and rates of falls (2.2% vs 0.5%, p=.22) and new or worsening pressure injuries (0.4% vs 0%, p>.99) were similar.
Conclusions: While our MOBILE intervention was associated with higher rates of BMAT assessment and placement of activity orders among hospitalized older adults, we did not find any association with functional decline or other clinical outcomes. These findings might be explained by the suboptimal uptake of BMAT, inadequate intervention fidelity, or inadequate connection between intervention and effective behavior change (e.g., activity orders were placed but nurses may not have followed the order).