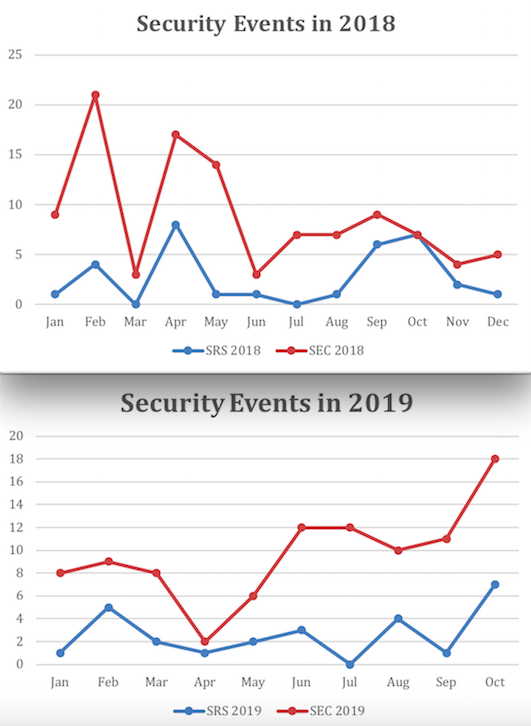
Background: Incidences of workplace violence have increased over the past decade and remain a major public health issue among health care workers. In response, there have been recent innovations in responses to perceived threats of violence in place of initiating a security emergency, i.e., “code grey,” which triggers immediate presence of hospital security at the patient bedside and often leads to escalation of violence. S.A.F.E. (S=Spot a threat, A=Assess the risk, F=Formulate a plan, E=Evaluate the outcome) Response System (SRS) is a new alternate security response system involving notification of clinicians, nursing leadership, and security to gather on the unit with the clinical nurse to identify and collaboratively address the etiology of the threat in a proactive manner. The SRS was implemented in our hospital in November 2014 and demonstrated a 40% reduction in nursing injury rates. However, uptake of the SRS among general medical units has been slow, with baseline data demonstrating of the 138 security events in 2018, only 32 (23%) were SRS events versus security emergency codes.
Purpose: To increase awareness and utilization of the SRS in place of a security emergency code on four 15-bed medical care units.
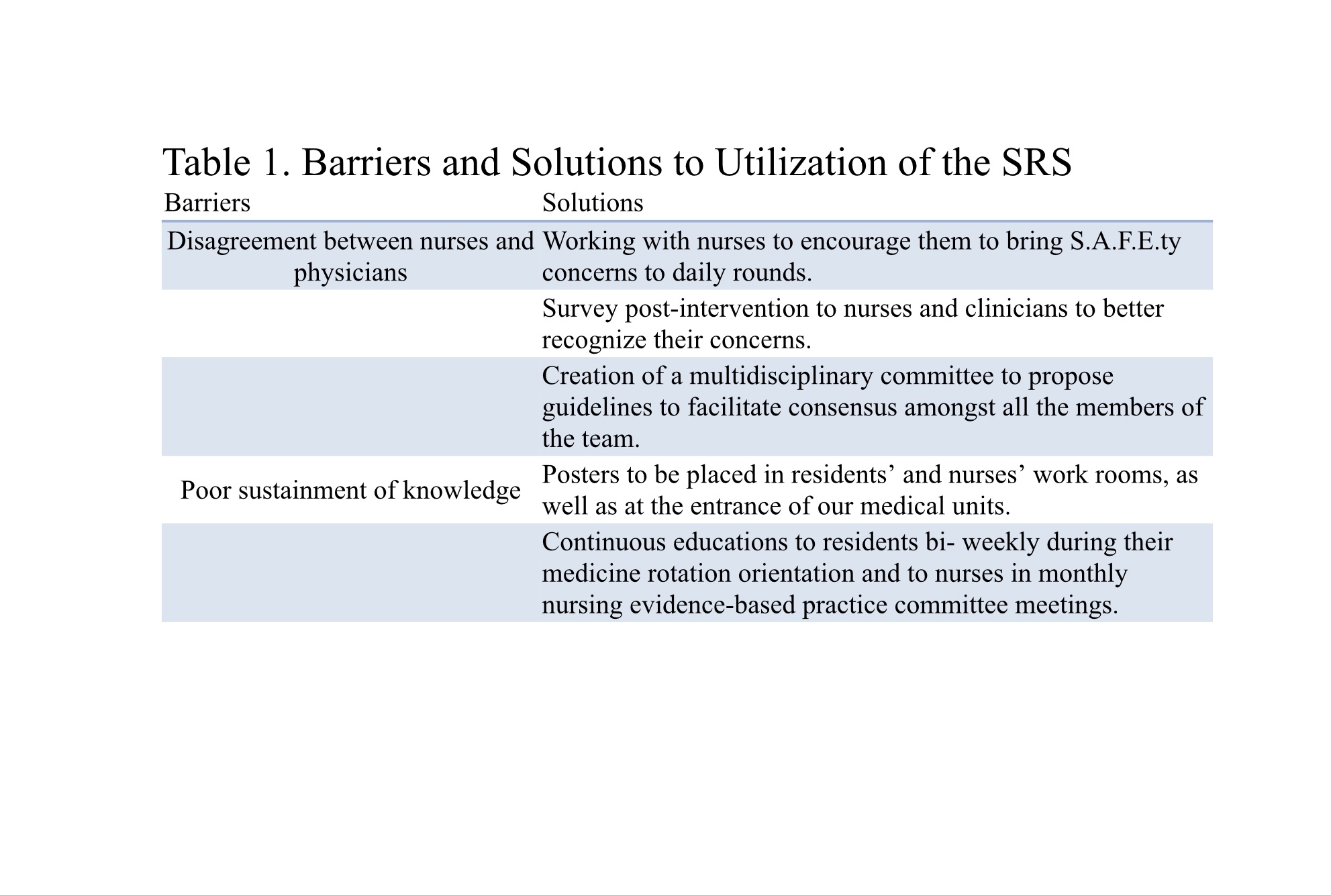
Description: We conducted a survey of clinicians (nurses, APPs, interns, residents, and attendings) to understand barriers to utilization of the SRS, which primarily demonstrated a lack of understanding of the difference between a security emergency code and a SRS. We, therefore, implemented a two-part initiative to address awareness including: (1) bi-weekly presentations during regularly scheduled CME conferences to resident and attending physicians providing education on the SRS policy; and (2) implementation of a “S.A.F.E.ty” checkpoint during daily weekday rounds to raise awareness and pro-actively identify potential safety threats. After a one-month wash-in period for implementation of the above interventions, we collected data on proportion of security events that were SRS events versus security emergency codes (August – October 2019). Our results demonstrate an initial increase in proportion of security emergency codes to SRS events from a baseline of 23% to 28% in only 2 out of 3 months after implementation. (Figure 1). Coincidentally, the hospital’s policy committee updated the SRS to include security leadership as part of the response team (not previously included) and created distinct response teams for inpatient versus ambulatory settings (November 2019). However, ongoing barriers to utilization of the SRS collected via focus groups demonstrated frequent disagreement between attendings and nurses on the type of security event to initiate during a perceived security threat, in addition to poor sustainment of knowledge of the SRS despite the described educational interventions (Table 1). We hope to address these in future refinement of this initiative.
Conclusions: We demonstrated that implementation of an educational initiative to improve awareness of the SRS may eventually be successful in improving utilization of this system in place of a security emergency code. We have identified ongoing barriers to utilization and plan to address these with ongoing interventions with an aim of achieving 50% use of SRS by June 2020. We hope this will help achieve our overall goal of maintaining a safe workplace environment for all healthcare providers.