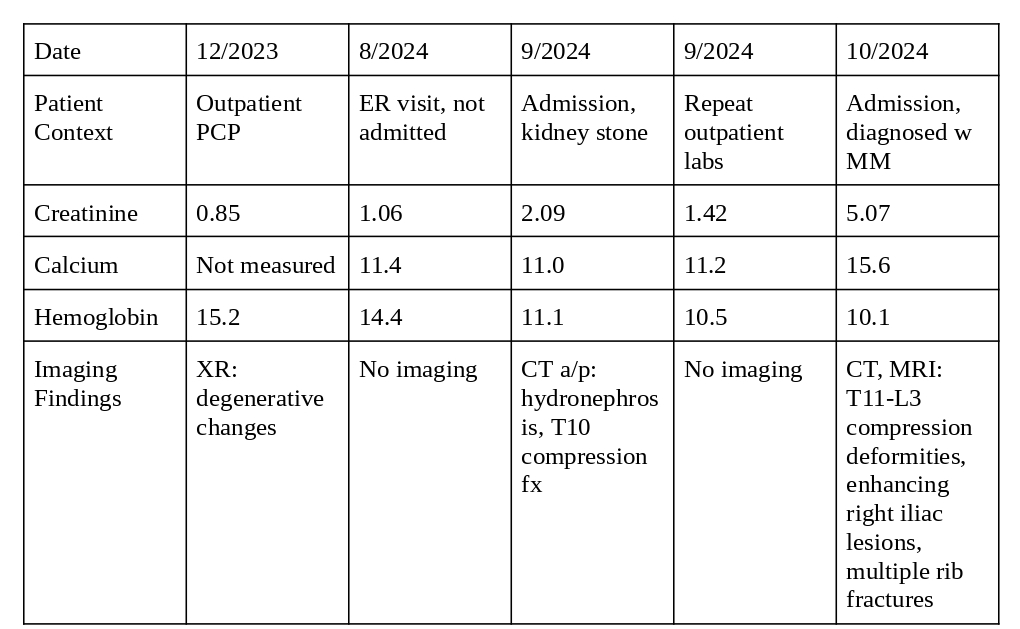
Case Presentation: A 67-year-old man with a history of chronic back pain from a motor vehicle accident (MVA) 20 years ago presented to his primary care provider for an annual visit in December 2023. He complained of persistent back pain. Lab work was unremarkable and an x-ray showed degenerative lumbar spine changes. The patient was recommended NSAIDs, physical therapy, and was referred to a spine center where he was prescribed a course of oxycodone.The patient’s back pain was treated conservatively at subsequent PCP visits. In September 2024, he presented to the Emergency Room (ER) with left colicky flank pain. Labs showed a calcium (Ca) of 11 mg/dL, a creatinine (Cr) of 2.09 mg/dL, and a hemoglobin (Hgb) of 11.1 g/dL. CT abdomen showed left hydronephrosis without nephrolithiasis and an age-indeterminate T10 compression fracture. He was admitted for an acute kidney injury (AKI) deemed to be post-renal from a presumed kidney stone. He was discharged two days later. His PCP obtained labs one week later, showing a creatinine of 1.42 mg/dL, Hgb of 10.5 g/dL. An iron panel was ordered.One month later, the patient re-presented to the ER with confusion, worsening atraumatic back pain, saddle anesthesia, and gait disturbance. Labs showed a Cr of 5.07 mg/dL, Ca of 15.6 mg/dL, and Hgb of 10.5 g/dL. CT and MRI revealed compression deformities from T11-L3, right iliac lesions, and multiple rib fractures. Bone marrow biopsy confirmed multiple myeloma. Given his extensive disease burden, the patient was transferred to an outside hospital for emergent chemotherapy.
Discussion: Multiple myeloma is a plasma cell malignancy characterized by hypercalcemia, renal injury, anemia, and lytic bone lesions, commonly known as the CRAB criteria. These symptoms can be difficult to associate given how common musculoskeletal pain and renal injuries are. In this case, multiple myeloma-induced renal dysfunction was masked by a post-renal AKI, and symptoms from lytic bone lesions were ascribed to a remote back injury.The renal injury was likely driven by both the stone and multiple myeloma progression, which is induced by light chain deposition, amyloidosis, and cast nephropathy [1]. The improvement in Cr was deceiving, representing a transient change from the passed stone and masking the underlying malignancy. In this case in the setting of anemia and AKI, serum and urine protein electrophoresis studies or beta-2-microglobulin could have led to an earlier diagnosis. This in turn can result in delayed disease progression, lower rates of complication (including compression fractures), and improved quality of life [2]. The level of clinical suspicion for multiple myeloma can understandably be lower in a patient with renal injury and chronic back pain, especially when other etiologies are present. The patient’s back pain was likely initiated by the MVA, but diagnostic momentum, validated by initial negative imaging, prevented the consideration of an additional, more acute process. The pain medications also masked the progression of lytic bone lesions, contributing to a delayed diagnosis.
Conclusions: This is a unique case of rapidly progressive multiple myeloma, demonstrated by changes in creatinine and calcium as well as compression fractures within two months. Common pathologies like kidney stones and chronic back pain can mask the CRAB symptoms, leading to delayed diagnosis and extensive disease spread. In diseases with limited life expectancy like multiple myeloma, early recognition is critical to preserve functional status and initiate chemotherapy.