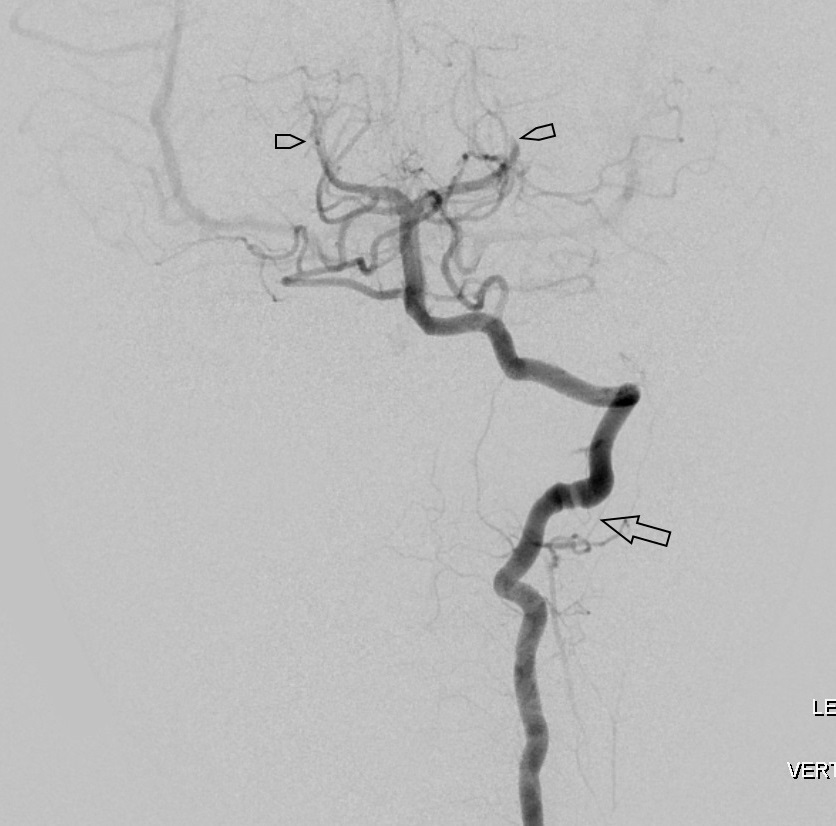
Case Presentation: A 5 year old boy presented with a 6 month history of headache (“my brain hurts”), vertigo, nausea and vomiting. No neurologic deficits noted on exam. MRI brain showed acute posterior circulation stroke involving the left cerebellar hemisphere and corpora medullaris. MRA head and neck were normal. Extensive work up evaluating for coagulopathic, autoimmune, infectious, cardiac, and metabolic disorders was negative. The diagnosis of cryptogenic stroke was made, and patient was discharged on aspirin. Symptoms of headache and vertigo continued, and cerebral angiogram was performed showing multiple arterial occlusions of the vertebrobasilar system and left middle cerebral artery concerning for thromboembolic disease. Also noted were wall abnormalities of the bilateral vertebral arteries at C1-C2 involving the interosseous segments. CT angiogram of the neck later confirmed bilateral arcuate foramina of atlas. This combination of findings was concerning for Bow Hunter’s Syndrome (BHS) or Rotational Vertebral Artery Occlusion Syndrome.
Discussion: BHS is a rare cause of vertebrobasilar insufficiency due to mechanical compression or tethering of the vertebral artery during rotation/extension of neck. Most cases are documented in adults, and only a few pediatric cases have been reported. In adults the syndrome often presents with intermittent vertigo, nystagmus, and ataxia. In children, most common symptoms reported are headache, vomiting and paresthesias. Most causes are due to hypertrophic bone spur or other osseous vertebral anomalies (including arcuate foramina of atlas). These anatomic defects cause stasis as well as shearing stress on the arteries, predisposing for thrombi formation. The gold standard for diagnosis of BHS is Digital Subtraction Angiography (DSA), a dynamic study which can show occlusion of the artery with head turning. DSA imaging in our patient showed luminal abnormality of the left vertebral artery at the level of C2. The congenital arcuate foramina were felt to be a source of tethering of the vertebral artery making them prone to stretch injury with head rotation. Patient was started on Lovenox and discharged home with neck collar, resulting in decreased frequency and severity of headache and eradication of vertigo. He underwent bilateral vertebral artery decompression and is currently in the recovery phase.
Conclusions: Acute ischemic stroke is rare in children, but has significant morbidity and mortality. Explicitly, posterior circulation stroke is uncommonly seen in the pediatric population, posing a diagnostic challenge for the pediatric provider. BHS should be considered in all cases of posterior circulation stroke, especially those associated with vertigo, ataxia, vomiting and paresthesias.