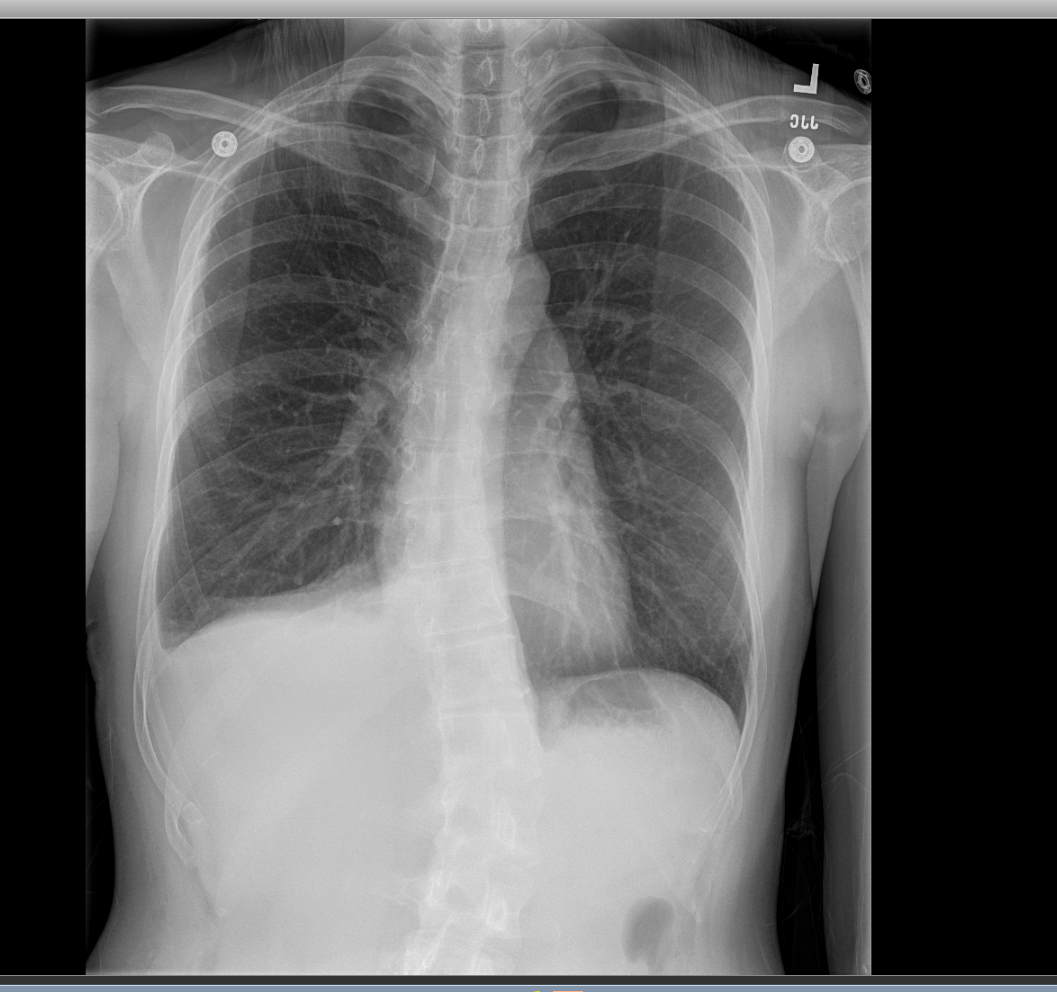
Case Presentation: A 37-year-old Korean female presented with 3-day history of worsening right posterior shoulder and chest pain, and exertional dyspnea. Review of System was otherwise negative. Past Medical History included chronic hepatitis B and an episode of pneumothorax 1 month prior. Her LMP was 2 weeks prior to presentation. On exam, she was tachypneic with absent breath sounds in the upper right lung zones. Vitals were otherwise within normal limit. Chest X-ray revealed moderate to large right pneumothorax (Fig 1). Labs were unremarkable including a normal α-1 antitrypsin assay. A chest tube was placed. On day 2 of admission the patient had video-assisted thoracoscopic surgery (VATS) with mechanical pleurodesis. Multiple diaphragmatic defects with endometrial deposits were found. The chest tube remained in situ for the duration of the hospital stay and removed 24 hours prior to discharge (Fig 2). Pelvic ultrasound was unremarkable and she was started on oral contraceptive pills.
Discussion: We describe a case of catamenial pneumothorax presenting outside the recognized 72-96 hour perimenstrual window. The classical definition of catamenial pneumothorax is the recurrence of air in the pleural cavity in reproductive-age women without lung disease. Diagnostic Criteria include: appearance within 72 hours before or after the start of monthly menses, characteristic pleural lesions, right-sided, and concomitant endometriosis (2). Approximately 3-6% of cases of spontaneous pneumothorax can be attributed to catamenial pneumothorax. Our patient presented approximately 2 weeks after her last menstrual period, which is unusual. There have been a few reports of cases presenting up to 7 days before and after the start of menstrual flow (2,3) but incidence outside this time period is exceedingly rare. The pathogenesis of catamenial pneumothorax is still not well understood. Many mechanisms have been proposed: Increased prostaglandin F2 causing blood vessel constriction and bronchospasms, migration of endometrial cells producing diaphragmatic defects, lymphovascular microembolism with pleural defects, and diaphragmatic air passage (2,3). Treatment includes hormonal therapy +/- VATS.
Conclusions: Catamenial pneumothorax accounts for 3-6% of spontaneous pneumothorax usually occurring within 72-96 hours peri-menstrual period. It is reasonable to consider catamenial pneumothorax in any female of child-bearing age with spontaneous pneumothorax and no known medical history. Oral contraceptive pills are the treatment of choice with surgical intervention for recurrence.