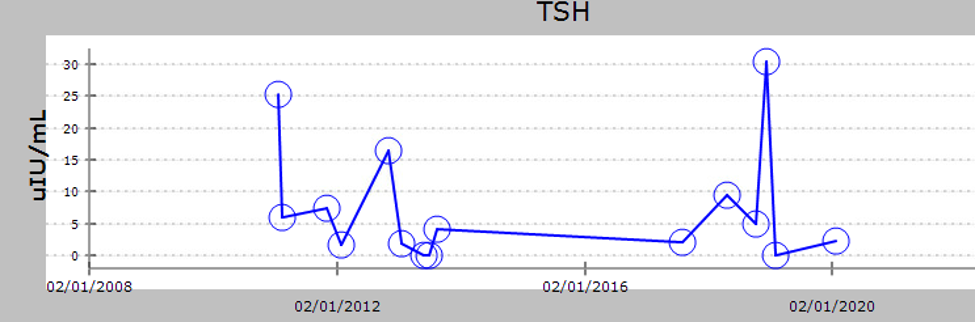
Case Presentation: A 44-year-old male patient with a history of vitiligo, presented with a chief complaint of lower extremity tingling and numbness sensation. Upon evaluation, the patient reported unintentional weight loss along with fatigue and frequent palpitation. A review of blood testing revealed an elevated TSH level, HbA1c, a low T4, Free T3, and vitamin B12. Anti-Glad antibody and intrinsic factor antibody were both detected along with antithyroglobulin antibodies. These results validated the diagnosis of Hypothyroidism, Type 1 diabetes mellitus, and pernicious anemia as the cause of B12 deficiency. Cortisol, ACTH, and Aldosterone were within normal. Calcium level and PTH were within normal limits for which possible hypoparathyroidism was excluded in this patient. Certainly, from the point of view of APS diagnosis and subtyping, this would be of key importance. Appropriate treatment was started.After some time, the patient presented to the office with a chief complaint of progressive worsening erectile dysfunction. Low free and total testosterone levels were accompanied by normal FSH and LH levels. Primary hypogonadism was identified as the cause. The patient was placed on testosterone replacement therapy upon ensuring the patient was not interested in fathering children at this time.
Discussion: Autoimmune Polyglandular Syndromes (APS) is an uncommon disorder with very varied manifestations, caused by the destruction of endocrine tissue leading to multiple endocrine gland failure, Patient can develop one or more of the following Type 1 diabetes, Graves’ disease, Hashimoto thyroiditis, Addison’s disease, vitiligo, alopecia, hypogonadism, and pernicious anemia. It can be classified into different categories depending on the glands involved. Autoimmune Polyglandular Syndrome (APS) has been classified into two different syndromes: Type 1 and type 2. There is also another type of APS which is characterized by two or more autoimmune endocrine organ destruction that does not fit the other types (either called type 2B or type 3). APS-2b or 3 is defined by the lack of Addison’s disease and the presence of autoimmune thyroid disease together with one of the other organ-specific autoimmune diseases, such as type 1 diabetes mellitus, vitiligo, and primary hypogonadism (female > male). Immunopathogenesis of the disease includes a cell-mediated immune process. Lymphocyte infiltration can lead to functional loss of the targeted gland. Regarding treatment, treat each endocrine gland dysfunction separately. Hormonal replacement therapy is the way to treat most endocrine disorders. However, Thyroid hormone replacement therapy can increase steroid metabolism by the liver, therefore, evaluate for adrenal insufficiency which is the most common and the presenting disorder in 50% of cases, between 69% and 90% of patients have circulating antibodies to 21-Hydroxylase.
Conclusions: Autoimmune Polyglandular Syndrome is a rare condition that should be taken into consideration when presenting with multiple symptoms that increase the likelihood of numerous endocrine gland involvement. It is rare but can be treated from the beginning to prevent any further destruction of the tissue or the development of gland scarring.