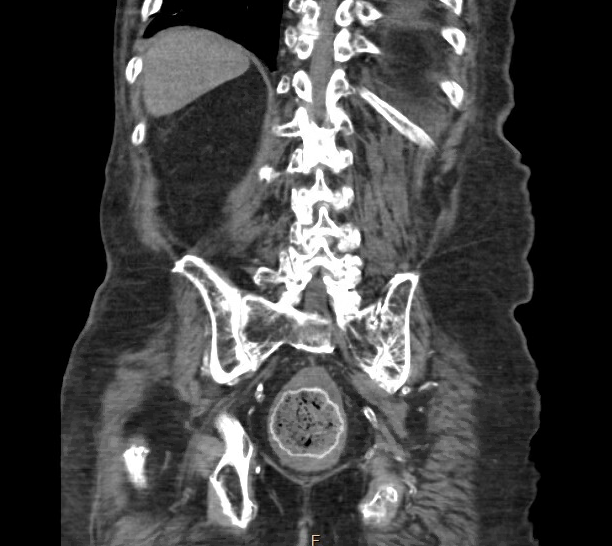
Case Presentation: A 77-year-old male with a past medical history of Parkinson’s disease, neurogenic bladder, and 2 episodes of partial colonic obstruction in the last 6 months presented with abdominal pain. Abdominal pain was intermittent, mild to moderate intensity, localized in the left lower quadrant, and his last bowel movement was 6 days ago. The patient had been having constipation with intermittent watery diarrhea for the past year. CT scan of the abdomen revealed findings suggestive of colitis along with fecal retention in the descending colon and a 9 cm lobulated mass with calcified rim-like density in the upper rectum. The patient had been daily self-catheterizing, hence an ingested or inserted foreign body was questioned which he denied. The patient presented with similar complaints multiple times during the past 6 months, and was offered colonoscopy for direct visualization of the suspicious mass, but had refused and opted for a barium enema instead. When comparing CT scans from the past 6 months, it was observed that the lobulated mass had intensification in the rim around it with migration from the distal sigmoid colon to the upper rectum. Due to concern about colorectal cancer with persistent symptoms, the patient agreed to get a sigmoidoscopy. Sigmoidoscopy revealed a 9 cm black-colored mass with egg-shell calcification around it, which appeared to be fecaloma. Mass was broken down with a water jet. Pathology confirmed stool material with calcium and barium salts in the rim without evidence of malignancy.
Discussion: Gastrointestinal dysmotility is a common occurrence in the elderly population (2). Sometimes due to the subacute nature of these gastrointestinal issues, such as constipation, diarrhea, dysphagia, dyspepsia, anorexia, and fecal incontinence, patients defer further investigations, while pursuing symptomatic treatment. (4)(5) Fecal impactions are frequently encountered in the setting of chronic constipation and anorectal anatomical or functional abnormalities like Hirschsprung disease, Colonic inertia, Outlet delay, and dyssynergic defecation. Elderly patients, patients with spinal injuries, and neuropsychiatric disorders are at the highest risk. Fecal impaction can lead to the development of fecaliths, which if severe can form fecalomas most commonly in the sigmoid colon and rectum. Symptoms include abdominal pain, overflow diarrhea, constipation, etc. Ingested calcium and barium salts from previous contrast studies can deposit around the fecalith giving the appearance of a radio-opaque rim around it. (1) Differentials included cancerous rectal mass, giant fecaloma, and foreign body. Complications of fecaloma include intestinal obstruction, colonic ulceration leading to gastrointestinal bleeding, urinary retention, and hydronephrosis due to mass effect. The hardness of fecalith depends on the degree of calcification and further defines the treatment choice. Treatment options include the use of enemas, laxatives, and manual disimpaction. If these conservative measures fail, colonoscopic intervention with a water jet, mechanical lithotripsy, and rarely surgical removal may be required. (3)(5)
Conclusions: Fecaloma can have an odd radiological appearance due to the deposition of radio-opaque calcium and barium salts around it and mimic colorectal cancer or foreign body. Timely identification, with minimally invasive direct visualization techniques such as sigmoidoscopy/colonoscopy, can help with timely treatment, thus preventing complications.