Case Presentation: A 69-year-old Africa-America female presented with one month of worsening bilateral lower extremity swelling/edema. She was nonoliguric. She denied chest pain, orthopnea or dysuria. The patient was diagnosed with adult T-cell leukemia/lymphoma two months prior to admission. She was initially treated with interferon and lamivudine, which were stopped due to prolonged neutropenia. Then, she underwent two cycles of CHOP regimen, which was complicated with an episode of acute kidney injury, but it quickly resolved. Upon arrival, BP was 135/78. An examination revealed bilateral leg pitting edema 3+. Initial work up showed significantly elevated serum BUN and creatinine at 78 mg/dL and 3.9 mg/dL respectively. Hemoglobin was 8.2, MCV was 90.5. Albumin was 1.7.
Urinalysis showed albumin 3+, blood 2+, RBCs 8, WBCs 42. The patient was found to have severe nephrotic range proteinuria with a urine protein/ creatinine ratio of 10.7. High urine BK viral load, high serum BK viral load, and positive serum CMV load were detected. TSH, complements level, and PTH were intact. Anti dsDNA, ANA, ANCA antibodies, hepatitis panel, and HIV were all negative.
Ultrasound revealed increased echogenicity of both kidneys.
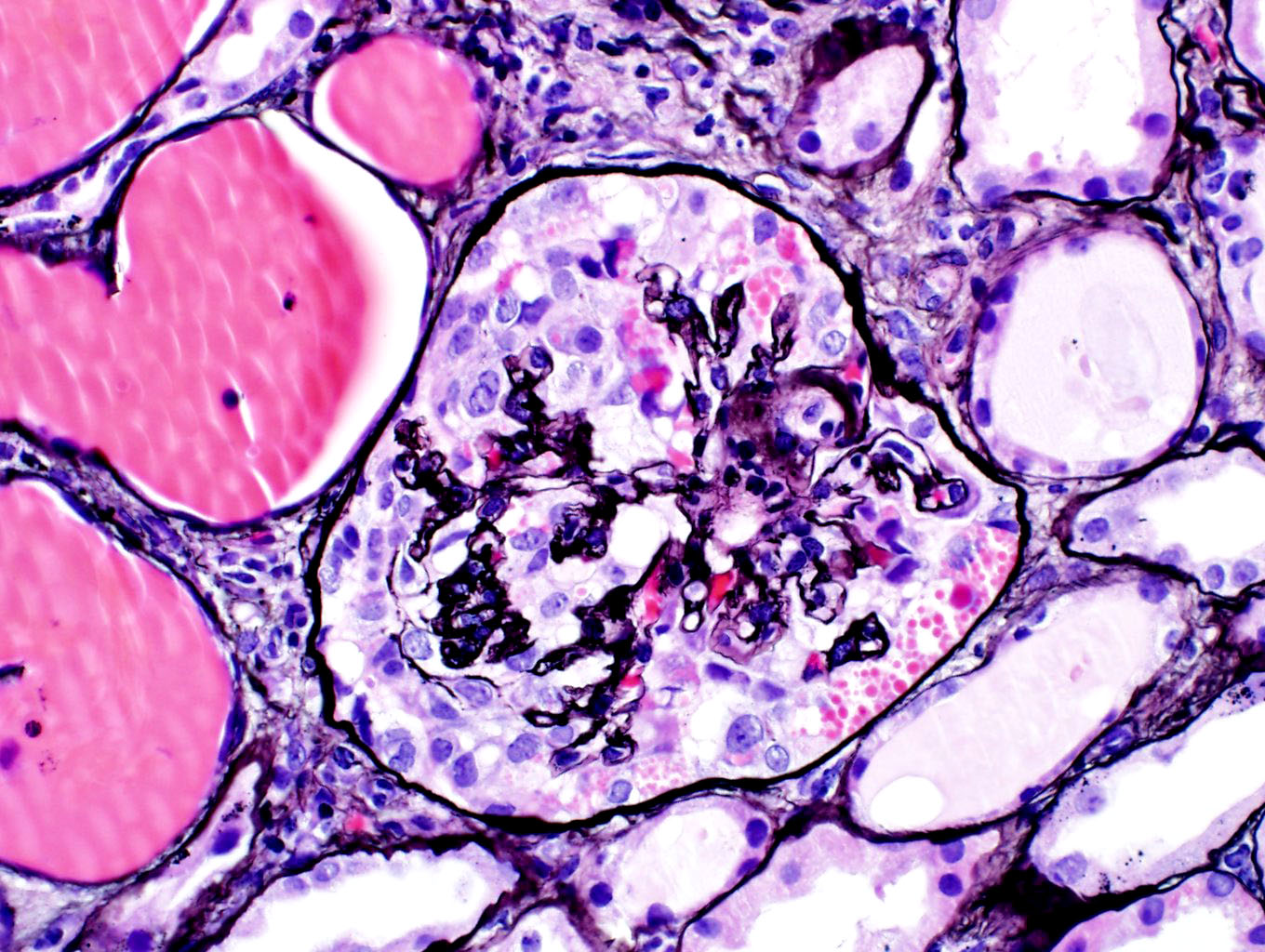
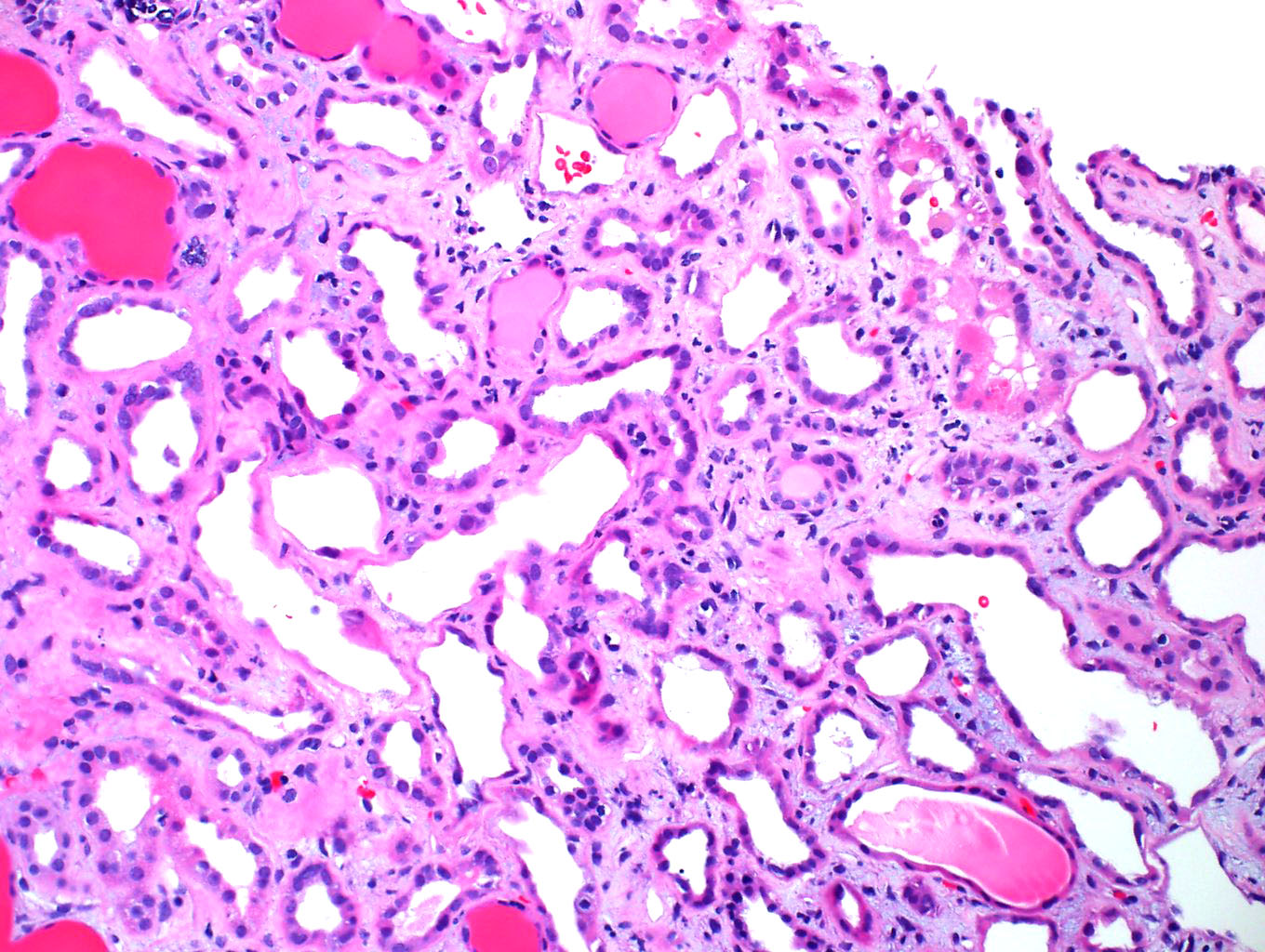
Kidney biopsy demonstrated collapsing glomerulopathy, moderate to severe tubular necrosis. And lymphocytic invasion and nuclei were noted in tubules suggestive of viral tubular invasion/nephropathy. SV40 and CMV staining were negative.
The patient received IV IG 2 g/Kg total dose in divided doses and Leflunomide 100 mg p.o. daily for BK virus associated nephropathy, and Valganciclovir for CMV infection. High-protein diet and protein supplements were offered. Three weeks of leflunomide and IV IG resulted in normalization of kidney function and improvement of proteinuria.
According to the time course and clinical scenery, a diagnosis of BK virus associated nephritic-nephrotic syndrome was made.
Discussion: Cases with BK virus associated nephrotic syndrome (BKAN) and collapsing nephropathy have been reported previously, in which immunosuppressive treatment resulted in renal failure and death or graft failure. There has been no defined treatment for BKAN. Recently, the use of the immunomodulant agent leflunomide, or IVIG together with the reduction of immunosuppression has been proposed.
This patient manifested as nephritic-nephrotic syndrome, with edema, positive urine RBCs and WBCs, hypoalbumemia and severe proteinuria. Kidney biopsy revealed tubular necrosis and collapsing. Lymphocytic invasion and nuclei were noted in tubules, which is suggestive of viral tubular invasion/nephropathy. The patient’s kidney function improved to her baseline at discharge, and her proteinuria significantly improved to 2 + after 2-3 weeks of anti BK virus therapy with IVIG and L. According to the time course and clinical scinenery, BK virus associated nephritic-nephrotic syndrome was diagnosed.
Conclusions: Our case illustrates that test of BK virus load should be kept in mind in patients with nephrotic syndrome, especially in these undergo immunosuppression. Steroids and other immunosuppressants should be avoided if high BK virus load is detected.