Background: The hospitalist position has exploded in recent years to become one of the largest single groups of physicians in medicine, increasing in size by 50% from 2012 to 2018. Many early career hospitalists have limited, if any, dedicated training for the role beyond their internal medicine residencies. Accordingly, new hospitalists may have greatly varying levels of familiarity with equipment and procedures for which they will ultimately be responsible. Having a baseline proficiency with these skills has even more importance for the nocturnist, who may care for patients as the sole attending hospitalist present in the hospital, with limited support from specialists or more experienced colleagues.
Purpose: The purpose of this faculty development initiative was to improve the comfort and preparedness of new nocturnists at our institution to supervise resident-led teams which run rapid response teams (RRT) and cardiac arrests while improving upon their skills to troubleshoot common problems encountered overnight. Though the Accreditation Council for Graduate Medical Education (ACGME) sets standards for acquisition of independent practice knowledge and skills in these situations through residency training, new faculty often report lack of preparedness from residency training for handling these situations without supportive oversight and may benefit from simulation training occurring in a low stakes environment that does not adversely affect patient care. Periodically revisiting this practice in a longitudinal fashion is further a means to reinforce good practice habits and mitigate skill decay for these infrequent but high-stakes situations.
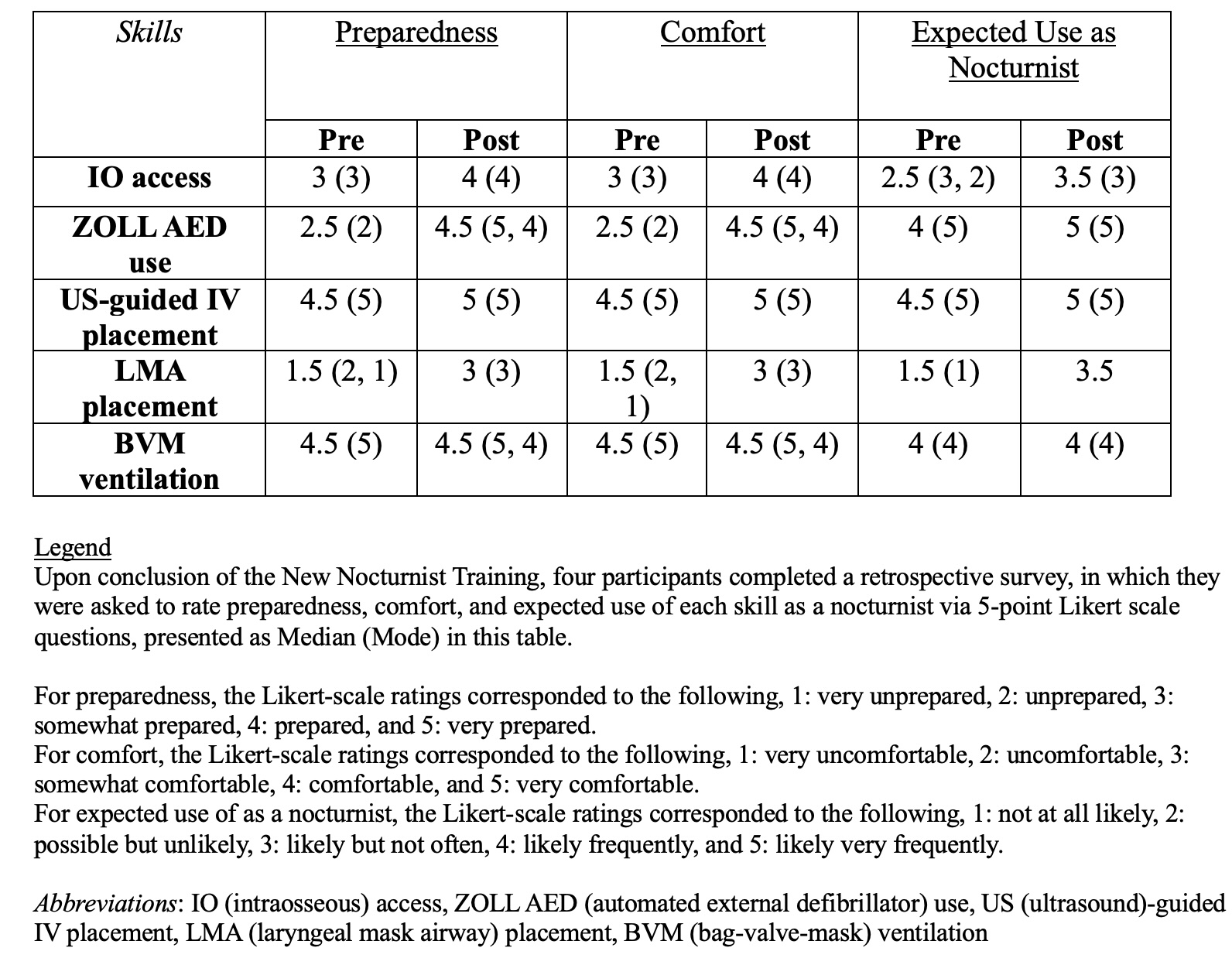
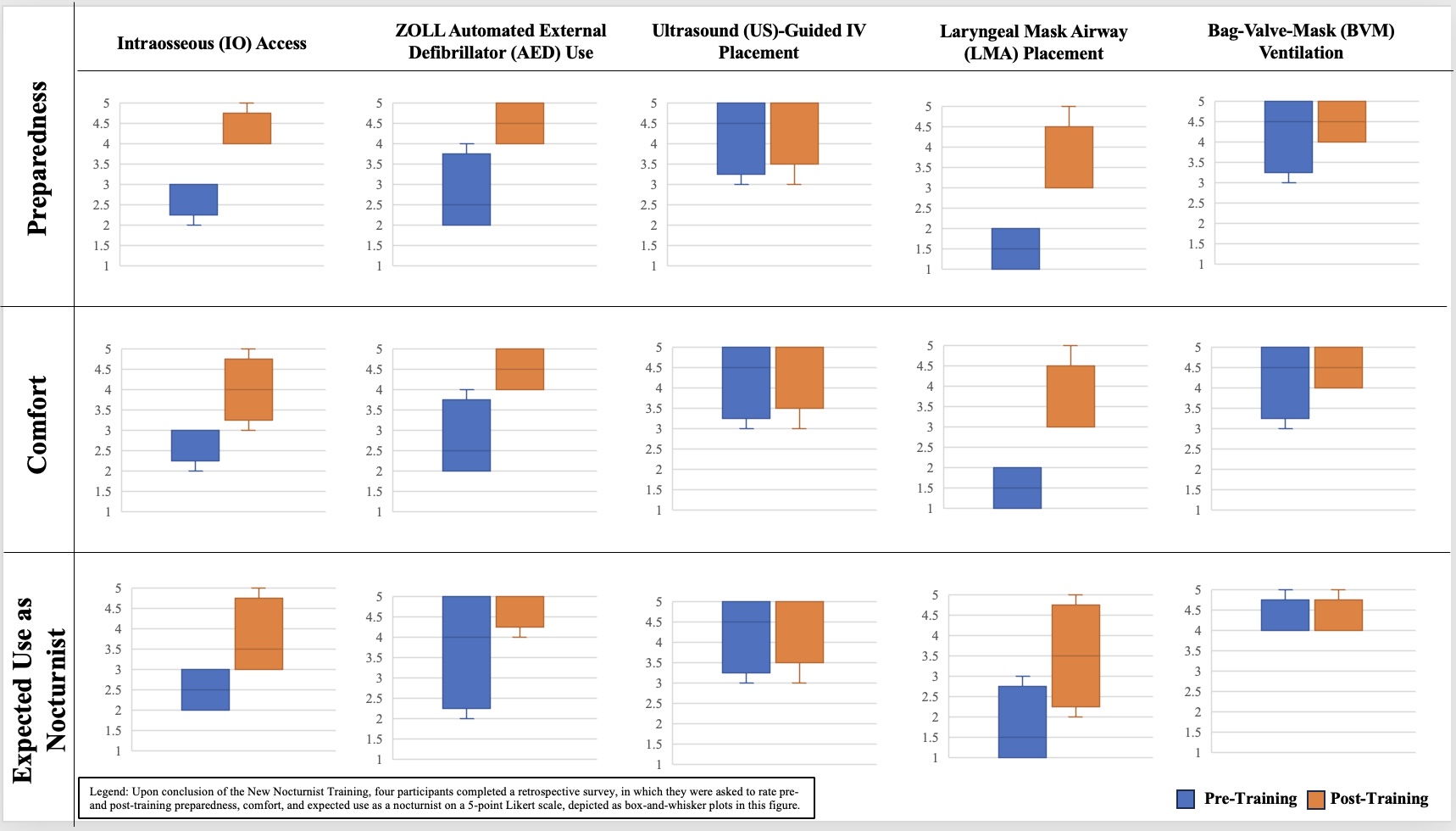
Description: This was a single-day hands-on simulation and skills-practice session with a cohort of new nocturnists prior to their start of clinical care responsibilities. Participants received one-on-one training with senior faculty in the following topics: obtaining intraosseous (IO) access, using a ZOLL automated external defibrillator (AED), placing an ultrasound (US)-guided IV, placing a laryngeal mask airway (LMA), and performing bag-valve-mask (BVM) ventilation. They then underwent simulated RRT and code practice as a collective, rotating leadership responsibilities, with simulations incorporating the practiced skills. At the conclusion of the training, they completed anonymous REDCap surveys to assess the impact of the training. Future sessions with this and new cohorts are planned for additional skills practice targeted to challenges encountered in real-life practice.
Conclusions: Four newly hired physicians participated in this pilot training. The median participant age was 33, and the median length of practice experience was three years. Pre-training, participants were most prepared and comfortable with US-guided IV placement and BVM ventilation; they expected to perform these skills, as well as ZOLL AED use, the most as a nocturnist. Post-training, the largest increases in median ratings for preparedness and comfort were observed for ZOLL AED use (Table 1). There were increases in median ratings for preparedness, comfort, and/or expected use as a nocturnist for all skills, except for BVM ventilation (Figure 1). In free text, all participants described the five skills as likely, very, or highly applicable for a nocturnist. These early survey results suggest that expanded implementation of our training modality could promote greater preparedness, comfort, and likelihood of use for high-yield skills among new nocturnists.