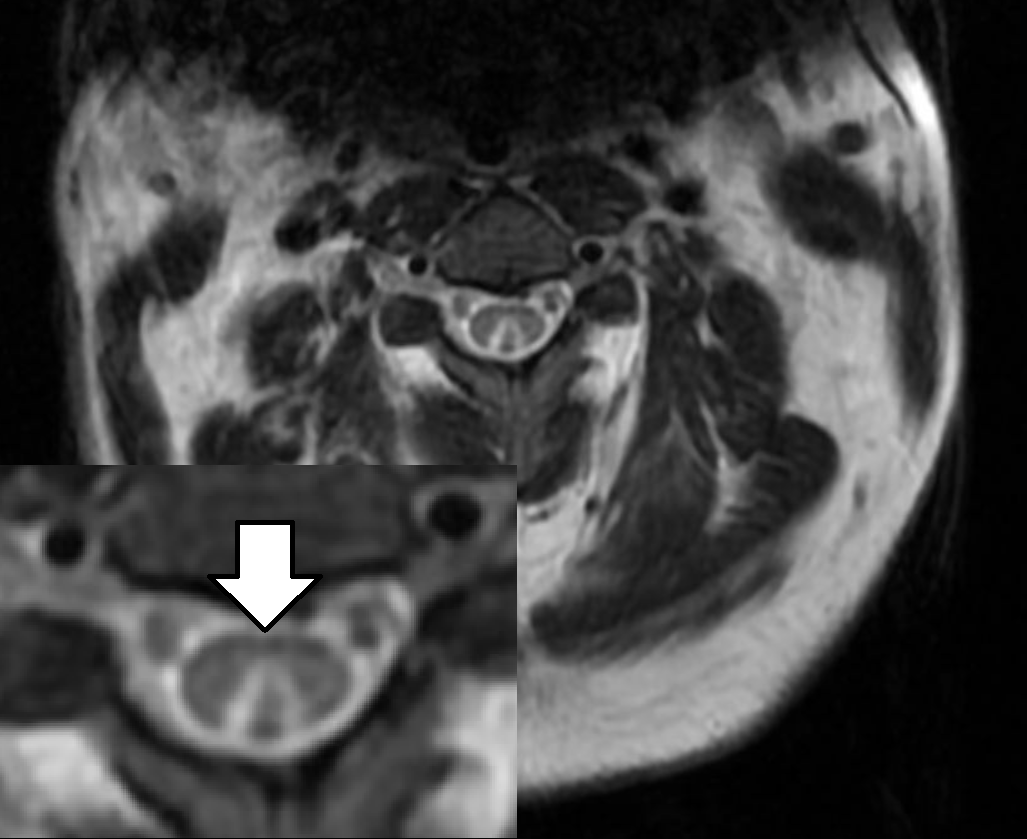
Case Presentation: A 34-year-old male with no past medical history was hospitalized for progressive weakness, numbness, and tingling of his extremities for 2 weeks. He denied fevers, headache, neck pain, or bowel/bladder complaints. He smoked 10 cigarettes and drank 24 to 48 oz beer daily. He admitted to social marijuana and cocaine use. He worked as a welder.Vital signs were normal. He had 4/5 strength in both legs and distal arms. Sensation to light touch was diminished in the distal extremities, and sensation to vibration was absent at both ankles and toes. Toe proprioception was diminished. CBC, BMP, LFTs, ESR, C-RP, and CK were normal. CT of the brain, cervical spine, and lumbar spine were normal. MRI cervical spine showed symmetric increased signal within the dorsal column.[Fig 1] Lumbar puncture yielded normal CSF. Infectious and autoimmune tests were negative.Vitamin B12 level was normal at 247 pg/mL, but methylmalonic acid (MMA) was elevated at 3.3 µmol/L and homocysteine elevated at 96 µmol/mL. The patient later admitted to recreational nitrous oxide (N2O) abuse on the weekends. He was treated with cyanocobalamin 1,000 mcg daily injections. PT and OT recommended acute rehab, but he was discharged to home due to lack of insurance. He was prescribed weekly B12 injections at discharge. Three weeks later, the patient reported partial improvement in his symptoms. He was independently ambulating and hoping to return to work.
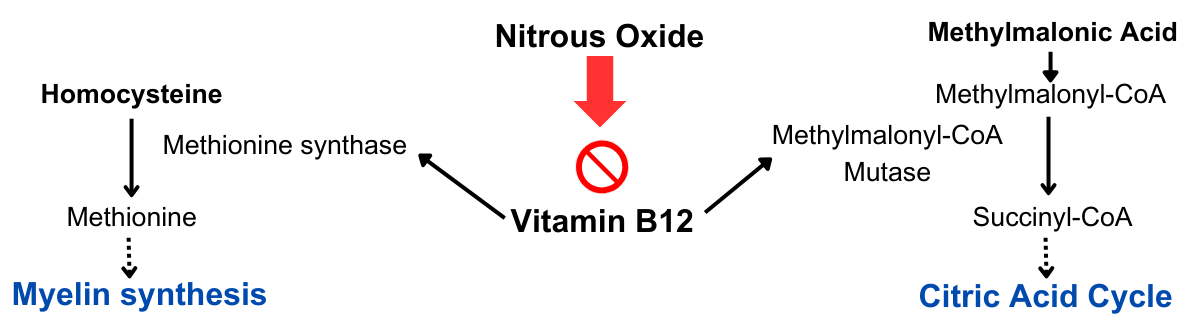
Discussion: N2O is a gas used clinically for anesthesia and in the food industry as an aerosol spray propellant. Inhalation may cause a rapid sensation of euphoria. Recreational abuse of N2O is increasingly prevalent, as it is easily accessible and legal to possess [1]. N2O inactivates vitamin B12, resulting in inability to produce myelin [Fig 2]. Subacute combined degeneration (SCD) of the spinal cord refers to demyelination of the dorsal and lateral spinal cord that can be caused by B12 deficiency. This patient had symptoms of SCD, including decreased vibration sensation and proprioception, paresthesias, weakness, and gait impairment. Most patients present with low B12 levels, but 30% may have normal levels. Homocysteine and MMA levels are almost always elevated (90.3% and 93.8%, respectively) [2]. SCD appears on MRI as “inverted V” shaped hyperintensity in the dorsal column on T2-weighted images [3], as seen on the patient’s MRI.SCD due to N2O toxicity is treated with aggressive B12 supplementation. There is no standardized regimen, but a common approach is initial frequent parenteral administration [4,5]. Outcomes of SCD vary, but most case reports demonstrated partial or complete recovery after treatment [6].For the hospitalist, this case offers valuable learning points. Screening for N2O abuse should be performed for at-risk individuals with abnormal neurologic symptoms. The diagnosis of N2O toxicity may be elusive, as the B12 level may be normal, and the differential diagnosis (including Guillain-Barre syndrome, transverse myelitis, multiple sclerosis, or other metabolic deficiencies) may lead to extensive testing. Early identification of B12 deficiency and the MRI findings of SCD can expedite treatment and recovery.
Conclusions: N2O causes neurologic impairment and SCD by inactivating vitamin B12. Abuse of N2O is widespread but may be overlooked by hospitalists. A thorough social history and proper interpretation of testing (including potentially normal B12 levels) are important to initiate prompt B12 replacement.