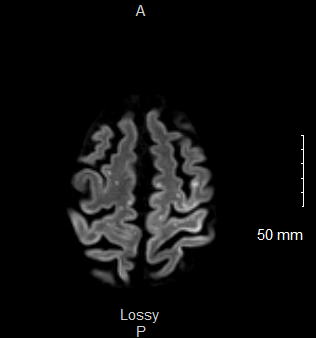
Case Presentation: Arterial air embolism is a serious condition that can lead to acute ischemic stroke. It is usually an iatrogenic process, during which air is introduced to the arterial system directly or through a pressure gradient. Although rare, air emboli can have drastic neurologic and cardiac complications and have been shown to be fatal in approximately 20% of cases. Here we present a rare case of cerebral air embolism (CAE) following administration of tPA into a PleurX catheter.A 79 year-old male with a history of squamous cell carcinoma of the left lung, recurrent left pleural effusion status post VATS with talc pleurodesis and PleurX catheter placement presented to the hospital with increasing weakness and confusion. On presentation, the patient was febrile with temp 101.1 F, tachycardic with HR 123, and hypoxic requiring 8 L supplemental O2. A CTA of his chest revealed left-sided hydropneumothorax with new pleural enhancement and thickening concerning for empyema. Cardiothoracic surgery performed pleural tPA administration to improve PleurX catheter drainage and obtain fluid studies. Immediately after the procedure, the patient became unresponsive. He was given Keppra and Ativan without improvement. CT imaging of the head was obtained promptly which was negative for acute findings. The patient was intubated for airway protection and was maintained on 100% FiO2 for a suspected air embolism. Continuous EEG did not confirm any seizure activity. TTE confirmed patent foramen ovale with strongly positive bubble study. Brain MRI ultimately showed multiple areas of T2 prolongation suspicious for acute infarcts from an embolic source. The patient had poor neurologic improvement and was ultimately transitioned to comfort care.
Discussion: The current case demonstrates a cerebral air embolism as a complication of bedside pleural tPA administration. Iatrogenic cerebral air embolism has been associated with surgical procedures and intravenous catheterizations, but cases associated with tPA administration have been described only a few times in the literature. This patient was at higher risk for CAE due to his patent foramen ovale. In his case, air introduction to either the pulmonary arteries or veins could ultimately deposit in the cerebral vasculature.Hyperbaric oxygen therapy has shown improved outcomes in patients treated within 6 hours of symptom onset though this is not readily available at all facilities. Administering 100% FiO2 via mechanical ventilation was associated with a higher removal rate of air from cerebral arteries, and it is an acceptable alternative when hyperbaric oxygen therapy is not available.
Conclusions: By describing this case, we are hopeful to raise clinical awareness among healthcare providers and to lower threshold for suspicion of air embolism when acute neurologic change is encountered following a procedure. Prompt recognition and management is essential for preserving neurologic function.