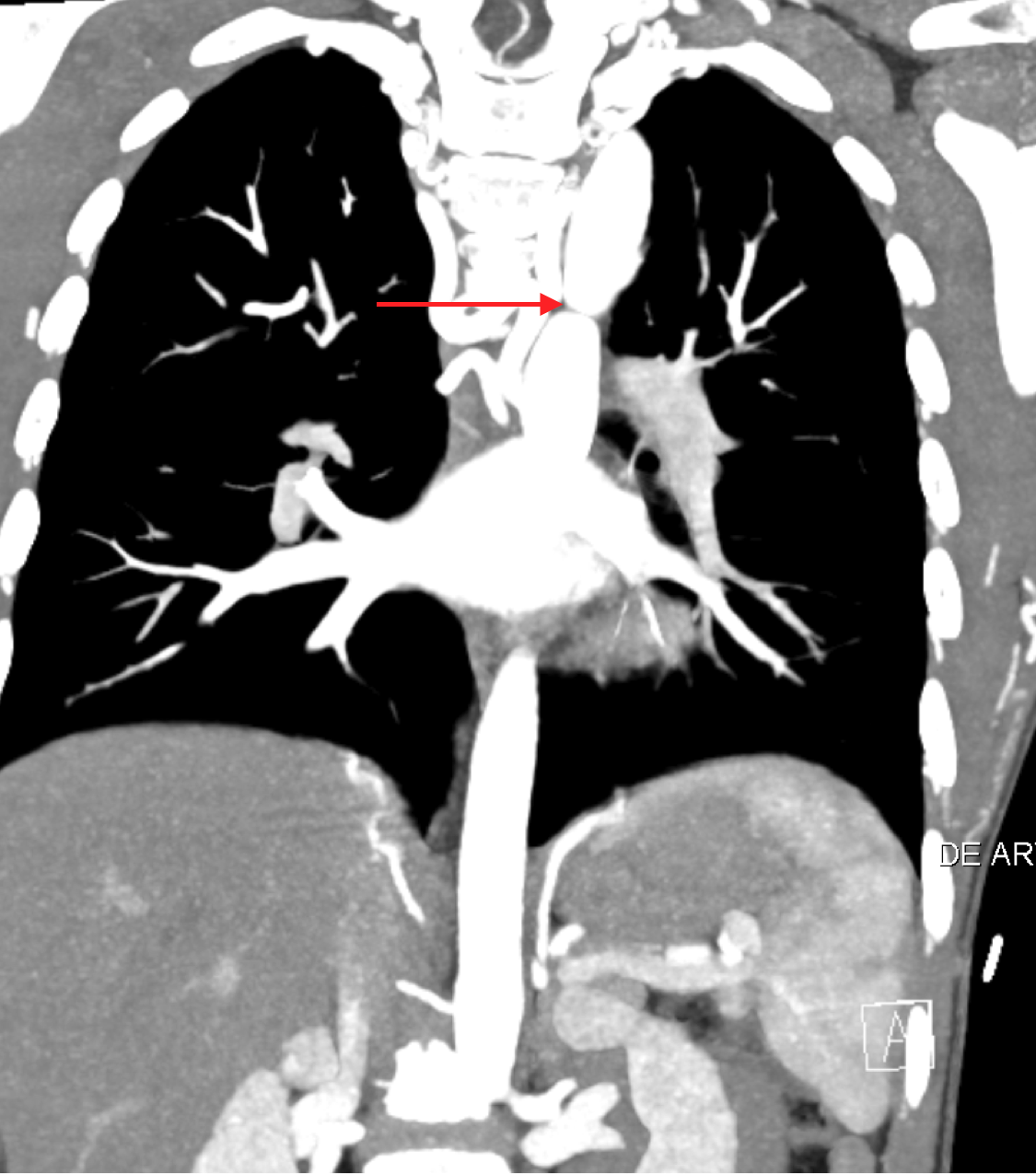
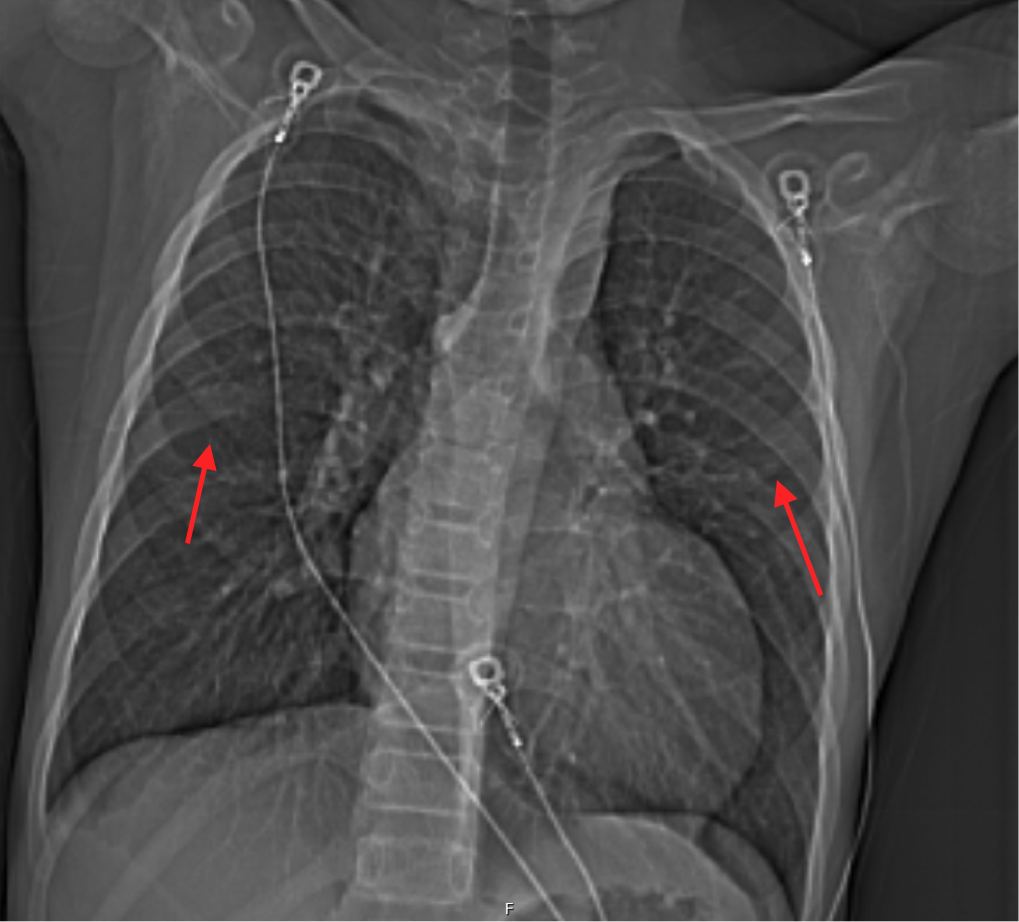
Case Presentation: A 12-year-old boy presents with 8 days of chest pain. He describes the pain as sudden onset, stabbing, located over his left chest with radiation to his right chest and left flank. The pain initially lasts between 5 to 10 minutes, but has been increasing in duration to span the entire day. The pain is associated with shortness of breath and palpitations. He denies any nausea, abdominal pain, diaphoresis, headache, or back pain. There is no known family history of arrhythmias, cardiomyopathy, seizures, congenital heart disease, or sudden cardiac death.On exam, he is nontoxic with a temp 36.6°C, HR 71 bpm, RR 17 bpm, BP 133/84 mmHg, and O2 saturation of 98% in room air. His height is 152 cm, weight 39.2 kg, for a BMI of 17. His heart is RRR with a grade III/VI systolic ejection murmur loudest over the LUSB, radiating throughout the precordium and to the back. Capillary refill is at 2 seconds. He has 2+ bilateral radial and carotid pulses, but no palpable pulses of the bilateral femoral arteries.EKG shows sinus rhythm with a prolonged PR interval of 196ms. CBC, CMP, and Troponin I are unremarkable. Echocardiogram reveals severe coarctation of the aorta, with inability to visualize the descending aorta, a bicuspid aortic valve, and a severely dilated aortic root. CTA chest show prominence of the great vessels arising from the aortic arch, severe narrowing of the thoracic aorta and prominent and numerous collateral arterial vessels (Figure 1). Notching along the undersurface of the posterior ribs is noted. (Figure 2)Diagnosis: Severe coarctation of the aorta (CoA)
Discussion: Most pediatric chest pain is not cardiac in nature. However, our patient had chest pain with murmur and non-palpable femoral pulses. This presentation makes CoA high on the differential.CoA is defined as a narrowing in the descending aorta. Clinical manifestations of CoA can vary depending on age. For all ages, a complete physical exam including palpation of four extremity pulses along with upper and lower extremity BP measurements is important. Delayed or absent lower extremity pulses can suggest a diagnosis of CoA. Initial evaluations include an EKG, which can be normal and a CXR, which may show notching of the posterior ribs from large collateral arteries. Most cases are confirmed with an echocardiogram. MRI or CTA scans can add complementary information about the anatomy and help with treatment and management plans. Balloon dilation and stenting is a safe and effective treatment for CoA in older infants and children.
Conclusions: Our patient underwent successful balloon dilation and stenting. He was started on aspirin and atenolol and has been doing well with no complaints. He continues to follow with pediatric cardiology, due to risk of re-coarctation and rebound hypertension with CoA.