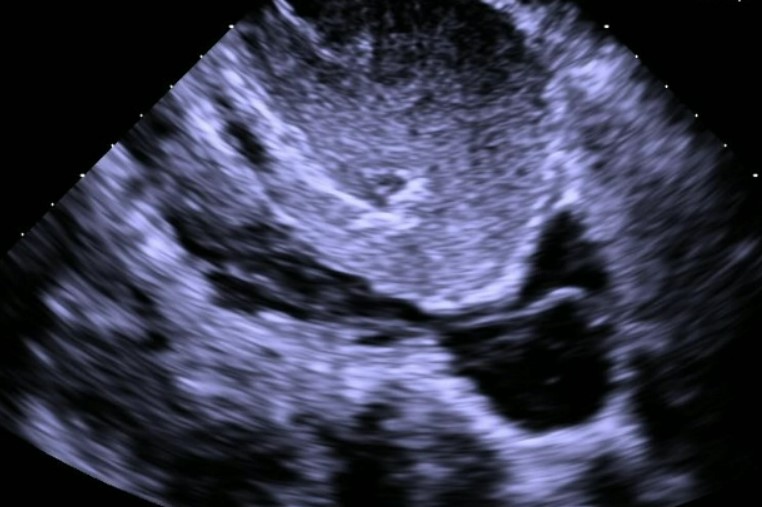
Case Presentation: A 51-year-old female with history of mitral valve prolapse, uterine cysts presented as a transfer from an OSH for evaluation of a right atrium (RA) and IVC clot vs tumor. She was admitted after screening echocardiogram (echo) showed possible clot in the RA. CT PE demonstrated possible mass vs multiple clots from the renal vein to the RA and IV heparin was started.OSH CT venogram reported thrombus vs tumor and MRI abdomen showed possible gonadal venous malformation. Our Interpretation of OSH images determined a hyperenhancing lobular structure in the IVC extending from the right gonadal vein to the RA, favored to reflect vessels rather than tumor or thrombus. Repeat CT chest/abd/pelvis confirmed enhancing structure consistent with tumor/webbing. Venogram and intravascular US showed connected cystic/webbed structure in the IVC extending up to RA. Repeat echo was concerning for IVC clot extending into the RA and across the tricuspid valve. Mass not active on PET and cardiac MRI found a cystic tumor with high fluid content.Multidisciplinary surgical evaluation was completed with plan to do hysterectomy and bilateral salpingo oophorectomy to obtain tissue sampling. However, surgery was deferred for 6 months due to possible clot. The patient was then discharged to a tertiary care center for a second opinion.Second opinion concluded with coordination of a single stage operation: total abdominal hysterectomy, bilateral salpingo-oophorectomy, midline laparotomy, full sternotomy with removal of RA/IVC/gonadal vein tumor with cardiopulmonary bypass support. Intra-operatively the tumor displayed mobility in the IVC and appeared spongy with smooth edges. No signs of thrombus or adhesions and the tricuspid valve and atrial walls were normal. The entire tumor was removed en bloc via the IVC and postoperative course was uncomplicated. Pathology was consistent with leiomyoma.
Discussion: Intravenous leiomyomatosis (IVL) and Intracardiac leiomyomatosis (ICL) are rare conditions with less than 400 cases documented in literature. Typical age of presentation is 50’s and common symptoms include dyspnea, leg edema, syncope, and palpitations. Surgical planning depends on presentation but single and two stage approaches are performed. Recurrence has been seen making long-term follow-up and repeat imaging imperative. Ma et al first described IVL into four stages: stage I: confined to the pelvis; stage II: tumor into iliac vein/IVC; stage III: tumor extending past renal vein, RA/RV; stage IV: tumor into pulmonary artery. Our case is consistent with stage III tumor with higher risk of cardio-pulmonary complications. Right sided heart failure, cardiogenic shock, and thromboembolism are associated with stage II-IV tumors. While we found IVL/ICL was a possibility, conservative 6 months of anticoagulation prior to tissue sample was chosen due to possible IVC thrombus associated with the IVL. Our case highlights care planning challenges in the setting of possible thrombus and the importance of surgical team consensus. Stage II-IV IVL/ICL requires prompt evaluation and intervention, with second opinions at times needed for the best outcomes.
Conclusions: Although rare, diagnosis of IVL/ICL should be considered in women presenting with DVT, a contrast-enhancing IVC or RA mass with a history of pelvic surgery, hysterectomy, or uterine leiomyomas. Surgical resection is usually curative, but requires multidisciplinary approach, highlighting the need for appropriate institutional capabilities and resources.