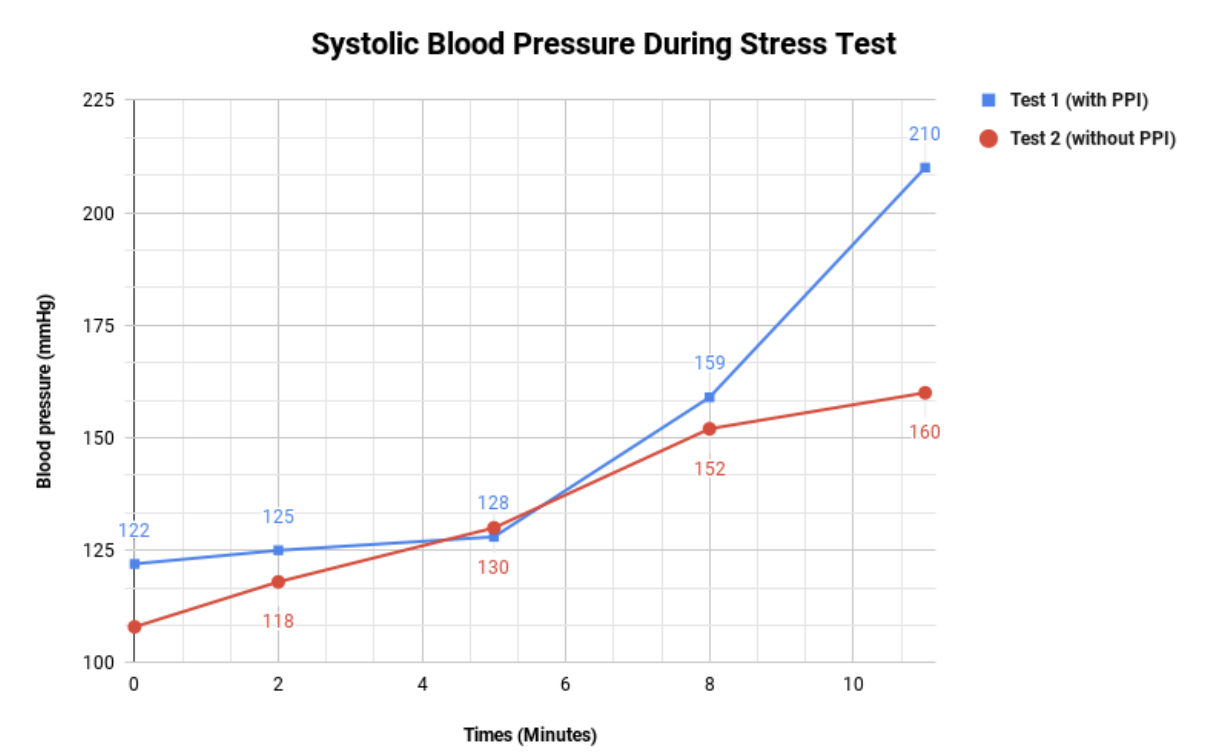
Case Presentation: The patient is a 52 year old male with a history of GERD on omeprazole therapy. In the period of one month, the patient developed significant exertional symptoms without any evidence of concomitant illness. The patient sought out further work up and evaluation by a cardiologist. Due to the presenting symptoms, an echocardiogram was performed which was largely unremarkable and showed an ejection fraction of 60%. Further workup was pursued with a stress test. During exertion, no ST segment changes were noted. However, once the patient’s systolic blood pressure reached 210 mmHg, up from 122 mmHg at baseline, he developed his typical symptoms. With these findings, the patient was diagnosed with exercise induced hypertension and managed with Amlodipine 2.5 mg daily, this provided minimal symptomatic relief. The Amlodipine was increased to 5mg daily and the patient reported minor improvement of symptoms. At this point, peak exertional blood pressure with exercise was measured to be 170 mmHg. His symptoms continued to persist despite therapy. Several months later, the patient discontinued the omeprazole due to gastrointestinal side effects. Within two weeks of discontinuation of the omeprazole, the patient noticed his exertional symptoms had resolved. He discontinued his Amlodipine, and a follow up stress test was done. During the subsequent test, the patient was able to exercise for a longer period of time and the maximum blood pressure recorded was 160 mmHg, down from the 210 mmHg during the first test. It was determined that his elevated exertional blood pressure was due to the omeprazole. He has began taking famotidine as an alternative treatment for his GERD symptoms.
Discussion: One explanation of the happenings described in this case is that omeprazole has been shown to interfere with nitric oxide synthesis. Nitric oxide (NO) is a potent vasodilator that plays a role in blood pressure. Proton Pump Inhibitors (PPIs) increase asymmetric dimethylarginine (ADMA) levels, they do so by inhibiting dimethylarginine dimethylaminohydrolase (DDAH) which is the enzyme that degrades ADMA. ADMA inhibits nitric oxide synthase and in return interferes with the overall production of nitric oxide. Decreased levels of NO can lead to increased blood pressure by leading to decreased vasodilation. This interference is the likely cause of the patient’s symptoms as evidence by the resolution of symptoms upon discontinuation of the PPI.
Conclusions: Prevalence in the general population is not known. However, given the number of patients taking PPIs it is likely underappreciated. While this may be most relevant in patients with coronary artery disease, particularly with ischemic symptoms, as experimental data shows that PPIs dysregulate vascular NO activity, these findings may be even more relevant in patients with subclinical cardiovascular diseases that are newly prescribed PPIs. Newly prescribed PPIs in a patient with subclinical cardiovascular disease may significantly increase their risk for progression of the disease. Ironically, patients with non-cardiac related chest pain are often times prescribed PPIs for treatment of suspected GERD which in return may lead to new cardiovascular symptoms. Consideration of alternative therapies for GERD may be appropriate for some patients with hypertension and coronary artery disease. This case highlighted the importance of appropriate medication management in patients with cardiovascular disease as many medications thought to be benign may actually pose significant risks.