Background: Immobility in the hospital setting is associated with persistent inability to perform activities of daily living, increased length of stay, and decreased return to independent living; this loss of function is identified by patients as a commonly unaddressed barrier to discharge. The reasons for immobility are multifactorial; however, lack of provider interest or value placed on mobility has been identified by patients, both locally and in published literature, as a barrier to their activity.
Purpose: Our primary aim is to create a resident-led interprofessional quality improvement initiative to improve patient mobility through enhanced patient-provider communication and goal-setting.
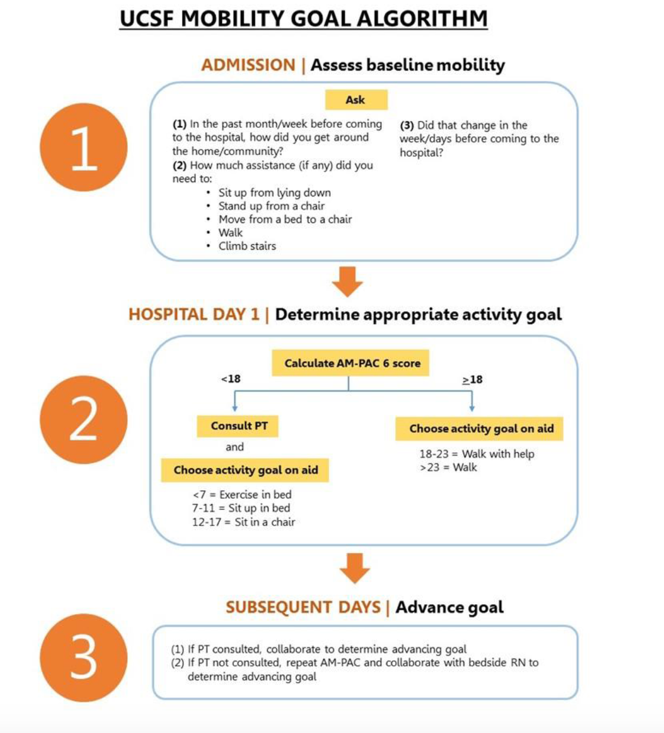
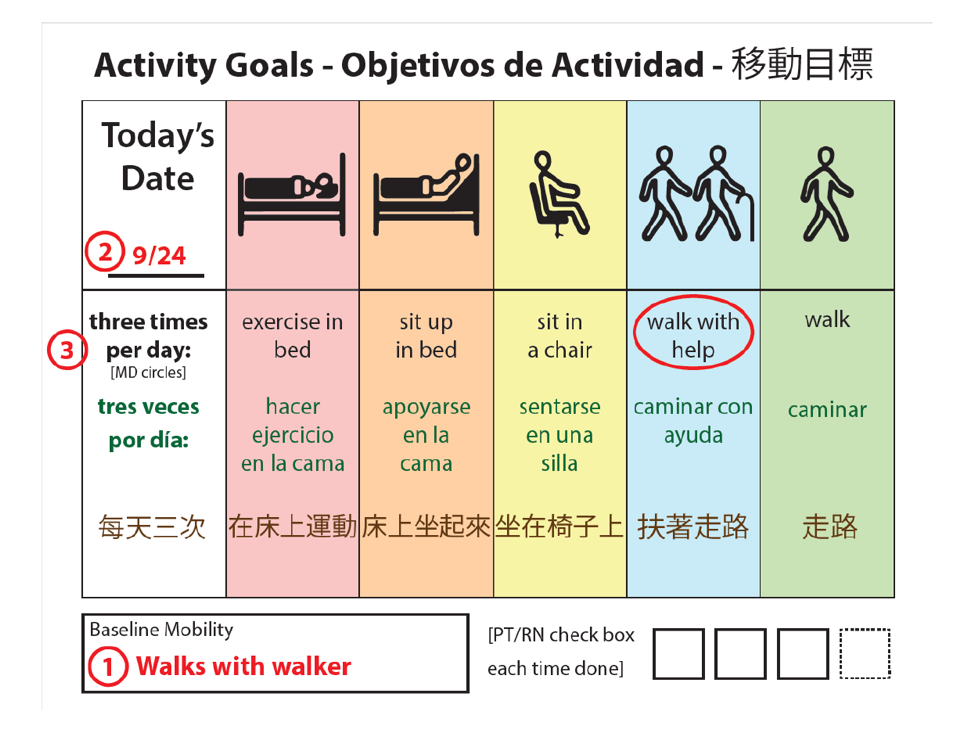
Description: This pilot program was implemented in October 2018 and is ongoing at a single urban academic medical center among Internal Medicine patients on a single unit. We developed a pathway that includes 1) Assessment of baseline mobility, 2) Selection of dynamic goals for in-hospital mobility, 3) Communication of this goal daily with patients 4) Collaboration with interprofessional team to support goal achievement. We employ a visual aid to encourage providers and patients to discuss baseline mobility, any current change from baseline, and select an appropriate activity goal (Graphic 1B). Baseline is assessed using the previously validated Activity Measure for Post-Acute Care “6-clicks” (AM-PAC) score. This tool scores patient mobility from a low score of 6 (total functional dependence) to a high of 24 (independent and unimpaired). An interprofessional team mapped AM-PAC scores to activity goals for patients (Graphic 1A), allowing for appropriate and dynamic goal setting. Programmatic measurement includes weekly audits of visual aid completion. Baseline patient-provider mobility communication was rare (2/14 patients, 15%); preliminary data from month 2 of implementation has revealed increased patient-provider communication (20/73 patients, 27%).
Conclusions: There have been several early lessons from this work: 1) Physicians do not feel ownership over mobility of their patients, 2) There is a significant knowledge and skill gap regarding mobility assessment and goal-setting among physicians, requiring enhanced provider education and interdisciplinary collaboration and 3) Patient-provider mobility communication is a small but vital cultural change within larger systemic modification necessary to promote activity among hospitalized adults.