
Background:
Acute lung injury (ALI) is a common cause of respiratory failure among hospitalized patients. Large studies have been limited to patients requiring mechanical ventilation, and little is known about non–mechanically ventilated adults with ALI. We sought to compare the clinical outcomes of non–mechanically ventilated patients with those of those requiring mechanical ventilation (MV) on day of ALI diagnosis.
Methods:
We evaluated all patients with ALI/acute respiratory distress syndrome (ARDS) enrolled in the Validation of Biomarkers in Acute Lung Injury Diagnosis (VALID) study, a large, multi–intensive care cohort. Mechanical ventilation status, s defined as the absence of MV on the day of diagnosis of ALI (day 0), was the predictor variable. We also evaluated requirement for MV within the first 3 days (days 1–3) of ALI diagnosis. Our outcome variable was in‐hospital mortality. Results: Of 685 patients with ALI, 137 (20%) did not require MV on the day of diagnosis. Our outcome variable was in‐hospital mortality. Results: Of 685 patients with ALI, 137 (20%) did not require MV on the day of diagnosis. Nonventilated patients had lower baseline morbidity and severity of illness compared with mechanically ventilated patients (Acute Physiology and Chronic Health Evaluation (APACHE) II mean, 22 ± 7 versus 29 ± 8); however, in‐hospital mortality was similar between the groups (26% in nonventilated vs. 23% in mechanically ventilated patients, P = 0.59). We found that 39 (28%) of initially nonventilated patients required MV within the subsequent 3 days of follow‐up, and although this subgroup did not differ according to age, sex, baseline morbidity, or severity of illness compared with the 98 other baseline nonventilated patients, they had significantly increased in‐hospital mortality (49%) compared with both the group requiring no mechanical ventilation within the first 3 days of hospitalization (16%) and the group that was ventilated on the day of ALI diagnosis (33%), P < 0.001. Severity of illness (APACHE II) accounted for the difference in mortality observed between the baseline mechanically ventilated group and those not requiring MV days 0‐3 (Table 1). However, the subgroup of patients nonventilated at baseline who went on to require MV in the subsequent 3 days had a fivefold increased adjusted odds of death compared with those not requiring MV days 0‐3 (Table 1).
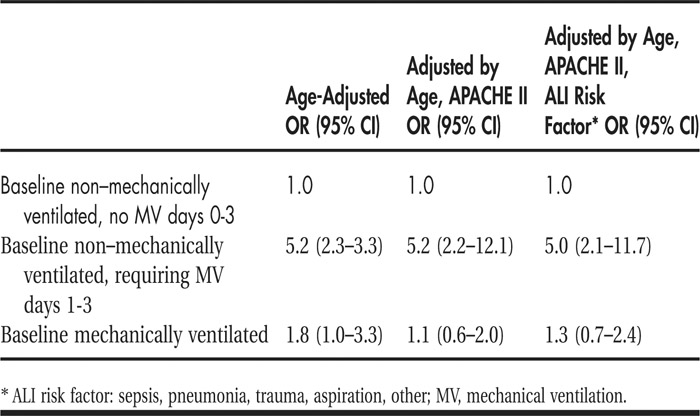
TABLE 1 Odds of In‐Hospital Death According to Mechanical Ventilation Status
Conclusions:
In a large, multi‐ICU cohort of patients with ALI, 20% of patients meeting ALI criteria are not mechanically ventilated on diagnosis. Although this group has a baseline lower morbidity and severity of illness, in‐hospital mortality does not differ. Furthermore, a subgroup of initially non‐mechanically ventilated patients with similar morbidity and severity of illness go on to require mechanical ventilation within the first 3 days of ALI diagnosis, and this subgroup has a significantly increased risk of in‐hospital death. This finding raises the question of how to identify these high‐risk patients earlier and whether earlier mechanical ventilation would affect the clinical outcomes of these patients.
Disclosures:
K. N. Kangelaris ‐ Society of Hospital Medicine Junior Investigator Award, research funding; C. S. Calfee ‐ K23 (NIH HL090833) and Flight Attendant Medical Research Institute, research funding; H. Zhuo ‐ none; M. A. Matthay‐NIH R37HL51856, research funding; L. B. Ware ‐ NIH HL081332 and HL103836 and American Heart Association Established Investigator Award, research funding