Background: Medication for opioid use disorder (MOUD) reduces mortality1-5 and is considered standard of care in all health care settings6, yet overall use of these life-saving medications remains low.7 Hospitalization represents a crucial opportunity to offer treatment and link patients to outpatient care. Patients who start MOUD during hospitalization are more likely to continue treatment after discharge and have fewer days of illicit opioid use.8-14 Factors such as housing insecurity and partner substance use make reaching these patients in other settings more challenging15. Hospitalist-led treatment can thus fill important gaps in care for patients with opioid use disorder (OUD).
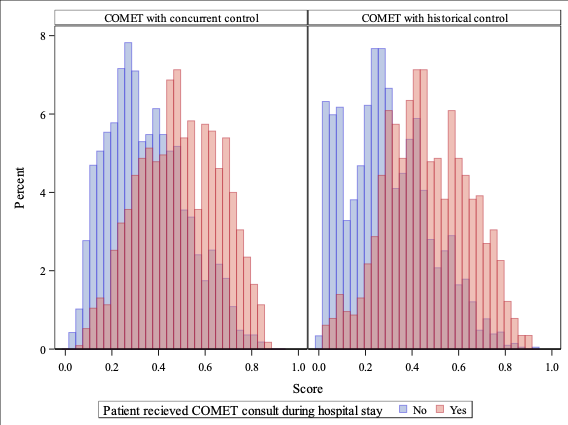
Methods: Project Caring for patients with Opioid Misuse through Evidence-based Treatment (COMET) is a hospitalist-led consult service which started July 1, 2019, with the primary aim of improving the care of hospitalized patients with OUD and/or opioid withdrawal.16 To evaluate the effectiveness of COMET, we conducted a retrospective observational cohort study utilizing electronic health record data for patients admitted to an academic medical center from January 1, 2016 through June 30, 2023. We identified encounters for adult patients admitted to Duke University Hospital with an OUD-related ICD-10 diagnosis code during their hospitalization. Propensity score overlap weighting was used to control for confounding by indication. Primary outcomes were determined prior to data collection and included MOUD receipt during hospitalization and 90-day mortality. As a more conventional metric, death within 30 days of discharge was subsequently added after data collection. Secondary outcomes included buprenorphine prescription, naloxone prescription, length of stay, 30-day readmission, and 30-day emergency department visit.
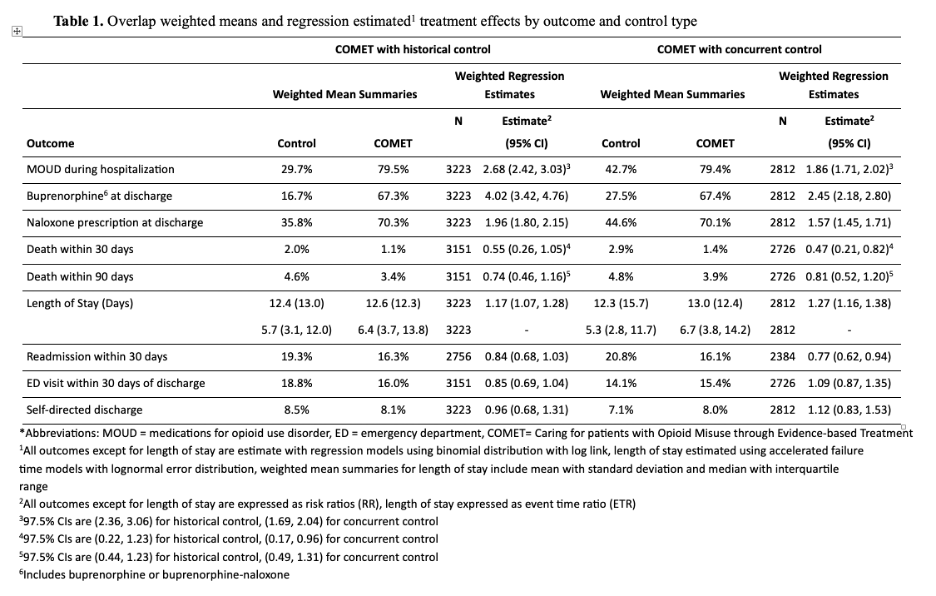
Results: There were 5,098 encounters for adult patients with OUD. Median age of patients was 42.3 years, 51.1% were female, 35.0% were Black, and patients were largely non-Hispanic (96.3%). Inpatient MOUD administration was higher for COMET patients with a weighted mean of 79%, compared to 29.7% of historical control (RR=2.68, 95% CI: 2.42-3.03) and 42.7% of concurrent control patients (RR=1.86, 95% CI: 1.71-2.02). Deaths within 30 days of discharge were less likely in those who received a COMET consult (RR=0.47, 95% CI: 0.21-0.82 for concurrent control; R=0.55, 95% CI: 0.26-1.05 for historical control). Association of COMET with post-discharge mortality lessened as the timeframe extended to 90 days (RR=0.81, 95% CI: 0.52-1.20 for concurrent control; RR=0.74, 95% CI: 0.46-1.16 for historical control). Readmission within 30 days was 23% lower for COMET patients compared to concurrent control (RR=0.77, 95% CI: 0.62-0.94). Compared to historical control group, there was a trend toward lower 30-day readmission rate for COMET patients (RR=0.84, 95% CI: 0.68-1.03). COMET did not have an association with rate of self-directed discharge or ED visits but was associated with longer hospital length of stay.
Conclusions: Most COMET patients received MOUD and were more likely to receive MOUD during hospitalization and at discharge compared to patients not seen by COMET. There is evidence that COMET patients had a lower risk of mortality and readmission within 30 days of discharge. A hospitalist-led consult service can improve care for hospitalized patients with OUD.