Background:
Hospitalized patients are at an increased risk of Venous Thromboembolism (VTE) and guidelines recommend risk assessment for all patients. The Padua score is one of several VTE risk assessment models and has 11 clinical components scored as either 1, 2 or 3 points. The most subjective component of the score is the reduced mobility assessment defined as “bedrest with bathroom privileges … for at least 3 days” which is difficult to operationalize and is assigned 0 or 3 points. Patients with a Padua score of 4 or greater are at risk of VTE. In our hospital, nursing completes the Padua score on admission as well as the Braden pressure ulcer risk assessment scale. The Braden Scale has 6 components and is widely used by nursing. One of the components is the activity scale which has explicit definitions (bedfast =1, chairfast = 2, walks occasionally =3 and walks frequently = 4). Lower points on the Braden Scale are predictive of a higher risk of pressure ulcers. Our study attempted to determine if there was alignment between the Padua mobility score and the Braden Scale activity score in the hopes substituting the straight forward and familiar Braden activity assessment with the more subjective Padua mobility assessment when risk stratifying hospitalized patient for the development of VTE.
Methods:
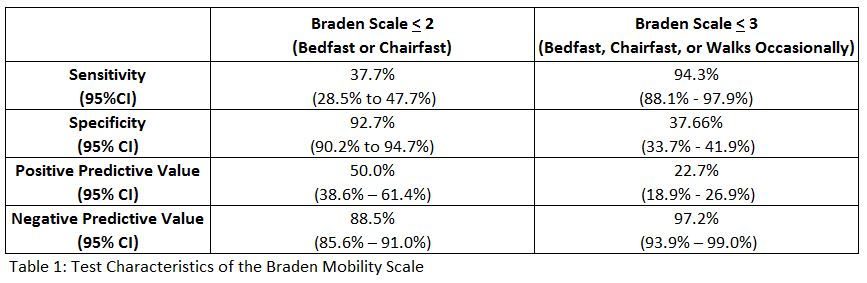
Retrospective chart review of 653 non-surgical, non-ICU, adult (age 21 and up) hospitalized patients who had both Padua and Braden scores completed on admission by nursing. Sensitivity, specificity, positive predictive value, negative predictive value, with 95% confidence intervals (CI) of Braden activity score of < 2 (bedfast or chairfast) vs. < 3 (bedfast or chairfast or walks occasionally) with Padua reduced mobility as the standard were calculated.
Results:
The prevalence of immobility by the Padua score was 16.2% (106/653). The positive predictive value for a Braden activity score of < 2 was 50.0% and was significantly better than (95% CI do not overlap) a score of < 3 (22.7%), however, both were low and would miss at least half of patients with a VTE risk factor. The negative predictive value of Braden < 3 was better than < 2 (see table).
Conclusions:
Our study shows poor alignment when a nurse assesses activity as a risk for pressure ulcers and mobility as a risk for VTE. Only half of patients assessed as confined to bed or chair were also assessed as having decreased mobility as defined in the Padua score. Although it is attractive to use an explicit and familiar evaluation of patient activity with the Branden Scale to predict decreased mobility, it is not sensitive or predictive enough to identify patients at risk, based on mobility, for VTE. Further research is needed to better define decreased mobility when assessing VTE risk.