Background: Hospitals are compelled by a variety of factors to optimize patient satisfaction. Pain management has been identified as an important determinant of overall inpatient satisfaction. However, effective pain management may be more challenging in the current climate of more cautious opioid use.
Purpose: The 32-item Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey dedicates two questions to pain management. We identified these two questions as our hospital’s poorest-performing patient satisfaction domain. This project sought to improve inpatient pain management as measured by the HCAHPS survey in a manner acceptable to providers and without increasing opioid adverse events. Our primary outcome was the average top box score on the two pain management questions. The top box score represents the proportion of patients who answer “always.” Based on the rate of improvement among the best-performing hospitals, we set a goal to improve the top box pain domain top box score by 1.2%.
Description: Project planning took place from July through November of 2016 during which time an interprofessional group of stakeholders was assembled, project scope was defined, and goals were set. That pain workgroup designed and subsequently undertook a multifaceted intervention over the following year. The intervention was made up of three major components. The first was a set of policy changes intended to simultaneously improve pain management practices and enhance safety. Parallel education of providers, nurses, and pharmacists was initiated in anticipation of the policy changes and continued in an ongoing manner thereafter. Finally, changes to individual medication orders and commonly used order sets were instituted to support best practices.
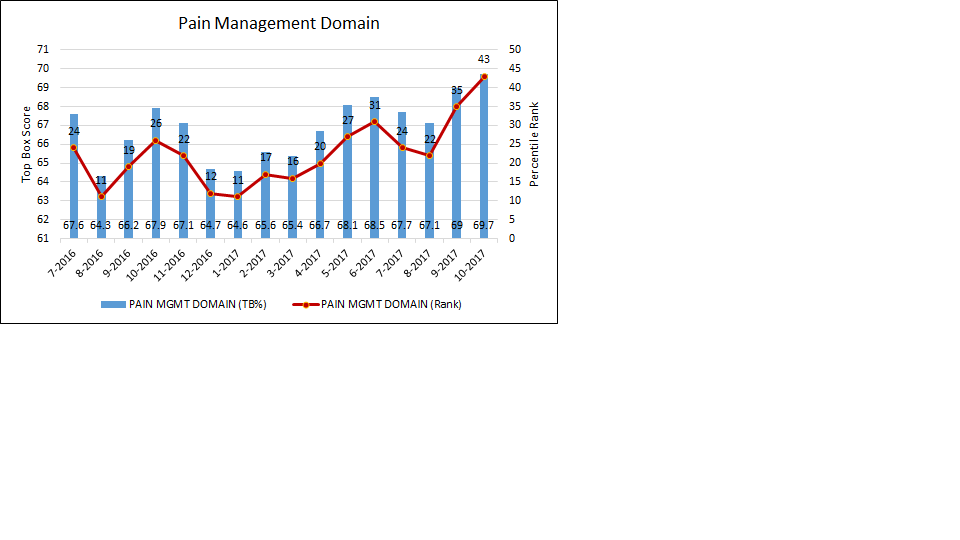
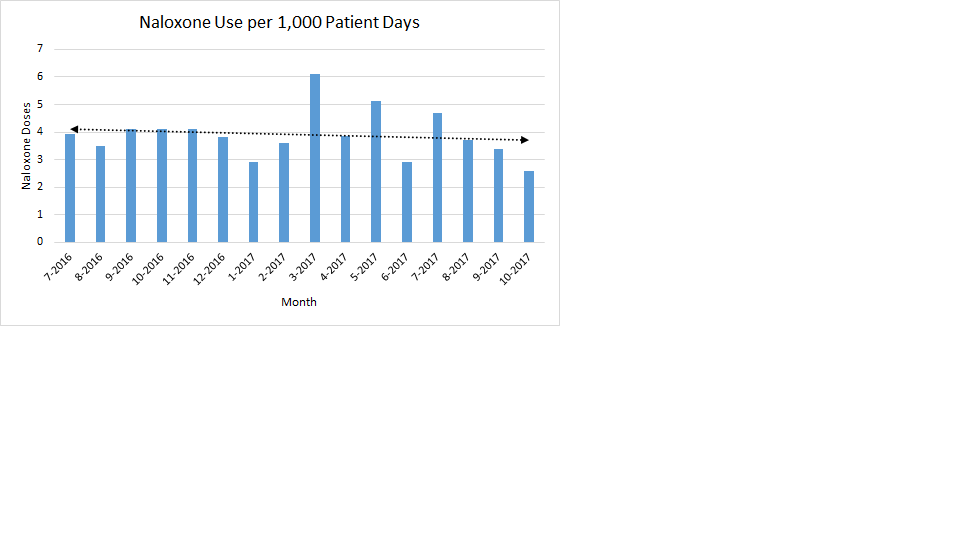
The top box pain domain score improved from 66.5% during the baseline period from July through October of 2016 to 68.4% over the most recent 4 months (July through October 2017). As depicted in Figure 1, the top box pain domain score continues to improve and reached 69.7% during the most recent reporting month. Despite the improvement in pain management, naloxone use declined over the same period from 3.9 doses (July through October, 2016) to 3.6 doses (July through October, 2017) per 1,000 patient days (Figure 2).
Conclusions: Scores on the HCAHPS pain management domain are not immovable and served well as a quality improvement outcome for this yearlong project. We were able to meet and exceed our goals for improving HCAHPS scores utilizing interventions designed to have minimal impact on opioid adverse events. In fact, several of our interventions aligned closely with best practice guidelines for reducing opioid overuse.
Keys to success
• Complete stakeholder representation
• Policy enhancements that support nurse responsiveness
• Modification of opioid order default options
• Enduring education
Improvements in pain management can be achieved in the current healthcare climate and may even complement efforts aimed at curtailing opioid overuse and preventing opioid-associated adverse events.