Background: Insurance companies are issuing more denials and causing financial instability for hospitals. On average, hospitals are paid $6,000 less for a patient in outpatient observation status as compared to inpatient status. According to Kaiser Family Foundation Health, the average expense in 2022 for a hospital per inpatient day was $3,025 and is only increasing. A recent report from the American Hospital Association and Syntellis analyzing data of 1,300 hospitals and health systems and found that Medicare Advantage (MA) denials increased by almost 56 percent. CMS has clarified that MA plans must follow the Two-Midnight rule. Despite patients having medically necessary hospital stays that exceed two midnights, some MA plans are still issuing denials based on InterQual criteria and MCG guidelines.
Purpose: With the strain from escalating denials that the insurance companies have placed on the healthcare system, it is more important than ever for a hospital to properly manage admission status. Because of this we partnered our physician advisors and our hospitalists to provide an automated, timely, and compliant screening of traditional FFS Medicare observation patients, which can be extended to MA patients with very similar expected results. The program ensures that Medicare patients requiring two medically necessary midnights in the hospital are discharged as inpatient status. Our physician advisors — experts in documentation, CMS compliance, and appropriate admission status — automatically review Medicare observation stays after one midnight. This allows the hospitalist to enter an inpatient order prior to discharge, which is required by CMS for FFS Medicare but is also a practical necessity for MA plans.
Description: To drive down the number of inappropriate long observation stays, we automated a process for all hospitalist patients with FFS Medicare and an order for observation services to automatically flow into the Sound Advisory nurse’s work queue. The Sound Advisory nurses watch those patients with an observation order (365 days a year). If they see any indication that the Observation patient is going to stay a second midnight (or the patient already has stayed a second midnight), then the patient will go into the Physician Advisor’s work queue. The physician advisors have read-only access to the EMR so they will go into the EMR and read all the notes, look at the vitals, labs, orders, etc. If they see medical necessity for inpatient level of care, they reach out to the hospitalist and request an inpatient order in real time.
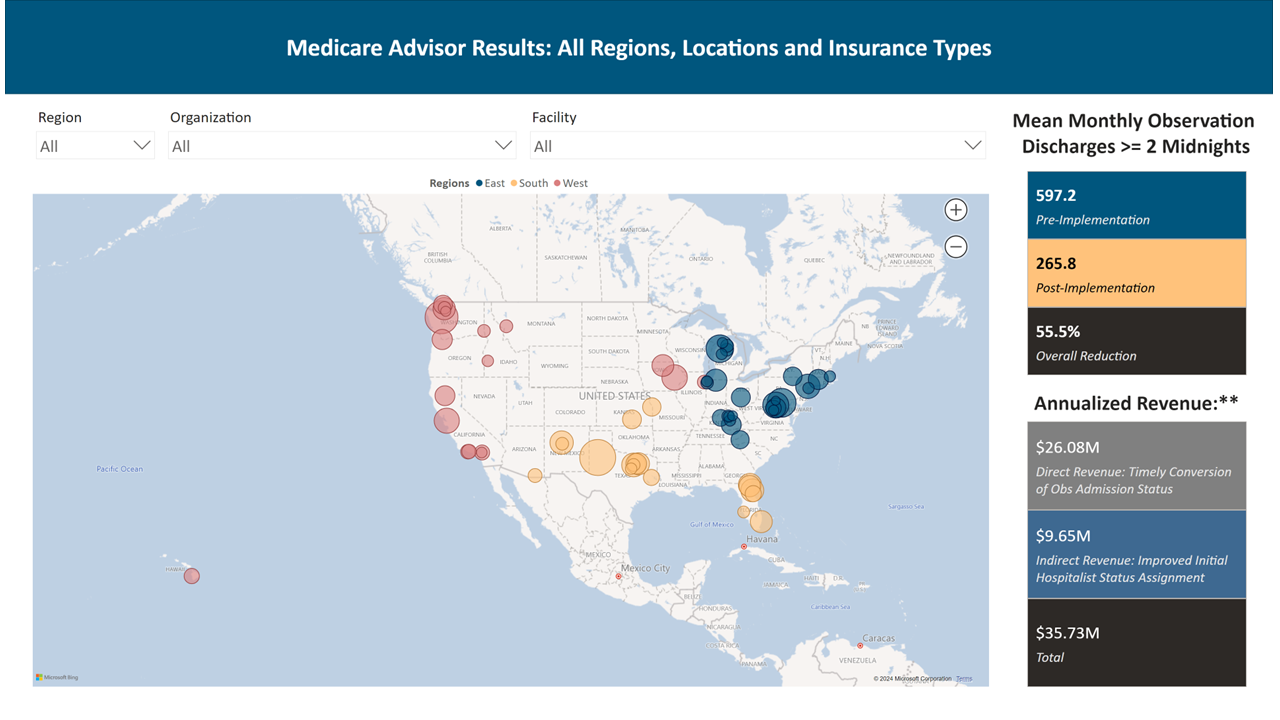
Conclusions: By implementing this process for FFS Medicare patients in 84 of our HM programs, we have been able to decrease Medicare long observation stays by 56%. Hospitals have seen an additional $35.74 million in annualized revenue just for FFS Medicare. As a proof of concept, we implemented the process at one Midwest hospital with 342 beds. We were able to increase their annual revenue for FFS Medicare patients by $384k and for MA plan patients by $438k. The MA plans did deny 20% of the cases where the patient remained 2 midnights but did not meet their screening tool (MCG or InterQual). We were able to turn over 80% of those denials just with our physician advisor doing a peer-to-peer discussion with the insurance medical director. Improving hospital revenue while maintaining compliance can be a challenge for any hospital. With our collaboration between our hospitalists and physician advisors, we have found a way to truly partner with the hospital to stabilize revenue and maintain compliance.