
Case Presentation:
A 45‐year‐old man with diabetes mellitus and hypertension presented with acute renal failure and multiple lesions on his penis and lower extremities. His presenting creatinine was 18, blood urea nitrogen 150, calcium 5.9, phosphorus 16.1, and parathyroid hormone 217 (12–65 normal). Hemodialysis was initiated immediately. He had a black ulcerated lesion on the tip of his penis, right thigh ulceration, and left groin abscess. Dermatology was consulted, and the differential included excoriations from pruritis secondary to the uremia. The penile lesions were thought to be secondary to ecthyma gangrenosum or vascular insufficiency. A vasculitis workup was unrevealing. Calcium phosphate product was initially elevated at 96 (>55). Pathology of the lesions revealed ischemic necrosis with microthrombi and calcium within the capillary walls, consistent with calciphylaxis. His lesions worsened despite initiation of hemodialysis and sodium thiosulfate. He developed autoamputation of the tip of his penis. Surgery and urology debrided his left groin abscess. The patient was a poor candidate for parathyroidectomy. Patient developed a sacral decubitus ulcer and an abdominal wall lesion from subcutaneous heparin. He suffered an aspiration event, an acute stroke with worsening of his calciphylaxis lesions.
Discussion:
Calciphylaxis is a rare disorder with significant morbidity and mortality. It affects up to 4% of patients with end‐stage renal disease. Penile calciphylaxis is even more rare, and the treatment is controversial: conservative wound care versus surgical debridement. The lesions are characterized as systemic medial calcification of the arterioles leading to ischemia and necrosis in increased areas with adipose tissue. Treatment options have limited efficacy but include wound care, reduction of calcium phosphate level by hemodialysis and sodium thiosulfate, and parathyroid hormone level reduction. An elevated calcium phosphate level (>55) or parathyroid hormone level can cause calciphylaxis with variability. Parathyroidectomy can decrease the disease progression. Subcutaneous injections can disrupt the skin integrity and lead to the development of ulcerations and progression to sepsis. Mortality rate is 50% in the first year and overall is 80%.
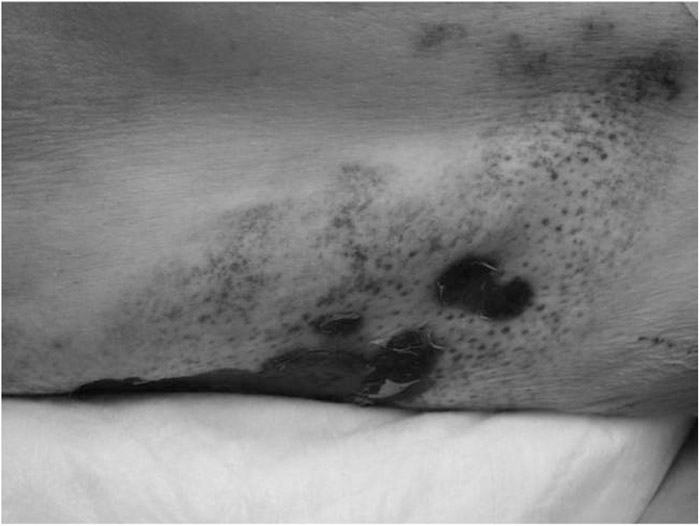
Calciphylaxis of right thigh with ulceration and eschar formation.

Necrotic glans penis with adjacent groin ulceration.
Conclusions:
Hospitalists care for many patients with end‐stage renal disease and need to be cognizant of calciphylaxis given its significant morbidity and mortality. Diagnostic evaluation and special care with skin integrity and treatments should be initiated immediately.
Disclosures:
S. J. Wang ‐ none