Background: Paracenteses are performed frequently at bedside by hospitalists, intensivists, gastroenterologists and emergency medicine providers. They are considered a core procedure that historically have been performed “blind” with only the use of percussion to determine the presence of fluid. With the rise of ultrasound based procedures the majority of paracenteses are now performed with ultrasound guidance. While the risks of these procedures are low, procedures are frequently performed on patients with abdominal varices, which may or may not be visible on physical examination. This puts patients at increased risk of bleeding, whether major or minor. A recent article by Brasuk, Rosen, Cohen, Feinglass, and Ault: ‘Vascular Ultrasonography: A Novel Method to Reduce Paracentesis Related Major Bleeding’ describes the use of a “two probe” technique. This technique involves first determining an appropriate site for needle insertion with a low frequency probe, followed by the use of a high frequency probe to evaluate for any blood vessels in the proposed needle path.
Purpose: Our bedside procedure service began using the two-probe technique in 2015 giving us the opportunity to validate the improved safety of the two-probe approach
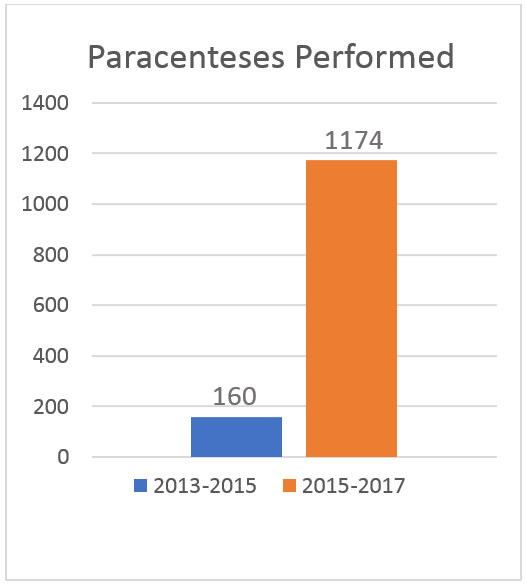
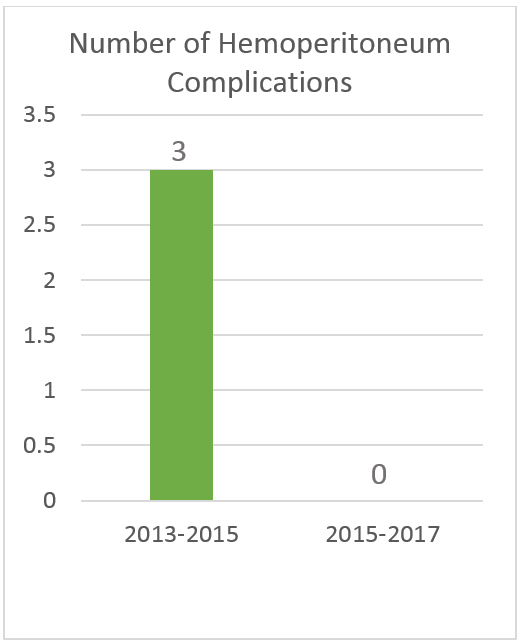
Description: Between 2013 and 2015 our service performed 160 paracenteses and had 3 hemoperitoneum complications. Between 2015-2017 our service performed 1174 paracenteses and had no hemoperitoneum complications. The average INR during the 2015-2017 year was 1.6, and the average platelet count was 134 thousand.
Conclusions: This direct comparison of the single and two-probe methods supports the improved safety of the two-probe approach in performing paracenteses, without adding significant skill or time burden.