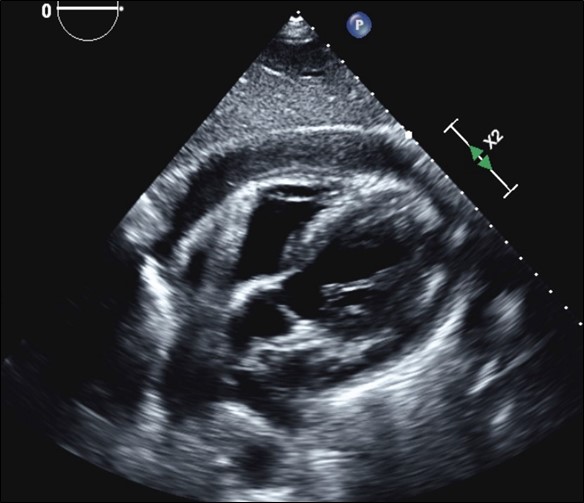
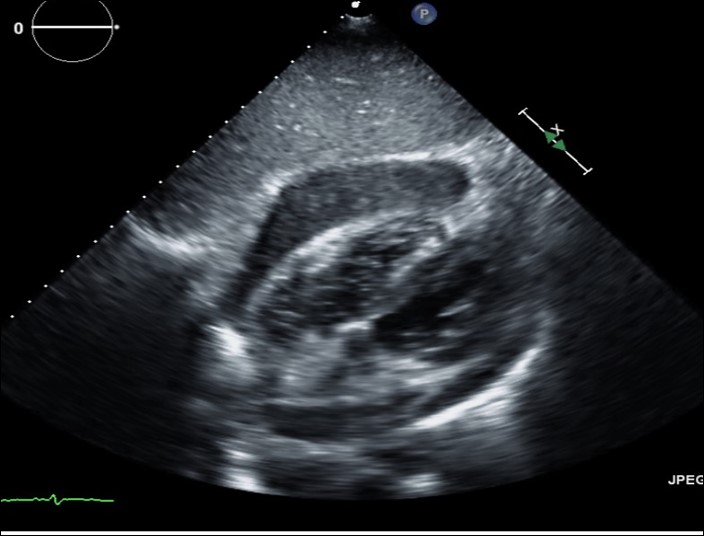
Case Presentation: A 63-year-old male with past medical history significant for uncontrolled diabetes mellitus type 2 presented with 4 days of chest pain and dyspnea. Patient was afebrile and vital signs were within normal limits. Lung and cardiac exam were unremarkable without cardiac murmur or rub. ECG showed ST elevations and troponins were negative. Left heart catheterization showed non-obstructive CAD not requiring intervention. Echocardiogram revealed small to moderate circumferential pericardial effusion without tamponade features. Initial blood cultures were negative. Repeat echocardiogram on hospital day 3 revealed increasing pericardial effusion without hemodynamic compromise. Hours later, patient rapidly decompensated, went into PEA arrest, and passed away. Repeat blood cultures collected prior to his death grew Staphylococcus aureus at 36 hours. Autopsy diagnosed acute suppurative and organizing S. aureus pericarditis with tamponade physiology as cause of death.
Discussion: Purulent pericarditis is a rare disease and is diagnosed post-mortem in more than 50% of cases. Diagnosis requires a high degree of clinical suspicion as mortality is almost 100% when treatment is delayed. Common causative organisms include Staphylococcus, Streptococcus, and Mycobacterium species. Predisposing conditions are immunosuppression, uncontrolled diabetes, chronic inflammatory states, and cardiac surgery. Clinical presentation is usually nonspecific with fever, chills, and tachycardia, often without chest pain or pericardial rub classically associated with pericarditis. Fever, cardiomegaly on chest radiograph, and elevated ST segments on ECG should increase suspicion for purulent pericarditis. Our case shows that significant purulent pericarditis can be present without positive blood cultures. The diagnosis is made predominantly by transthoracic echocardiogram which detects and quantifies the amount of pericardial fluid. Small to moderate pericardial effusions in hemodynamically stable patients are often monitored with serial echocardiograms unless diagnostic fluid sampling is needed, making the diagnosis of purulent pericarditis difficult to establish and delaying proper treatment. Complications include tamponade and constrictive pericarditis. Treatment is a combination of surgical and medical management with drainage of the pericardial fluid and antibiotics.
Conclusions: Purulent pericarditis is a disease with a high mortality that is easily missed as it presents with nonspecific symptoms including chest pain, fever, and pericardial effusion. Clinical deterioration and enlarging pericardial effusion should make a provider consider purulent pericarditis and prompt fluid sampling for diagnosis and treatment. Treatment requires both surgical drainage of the effusion and long-term antibiotics.