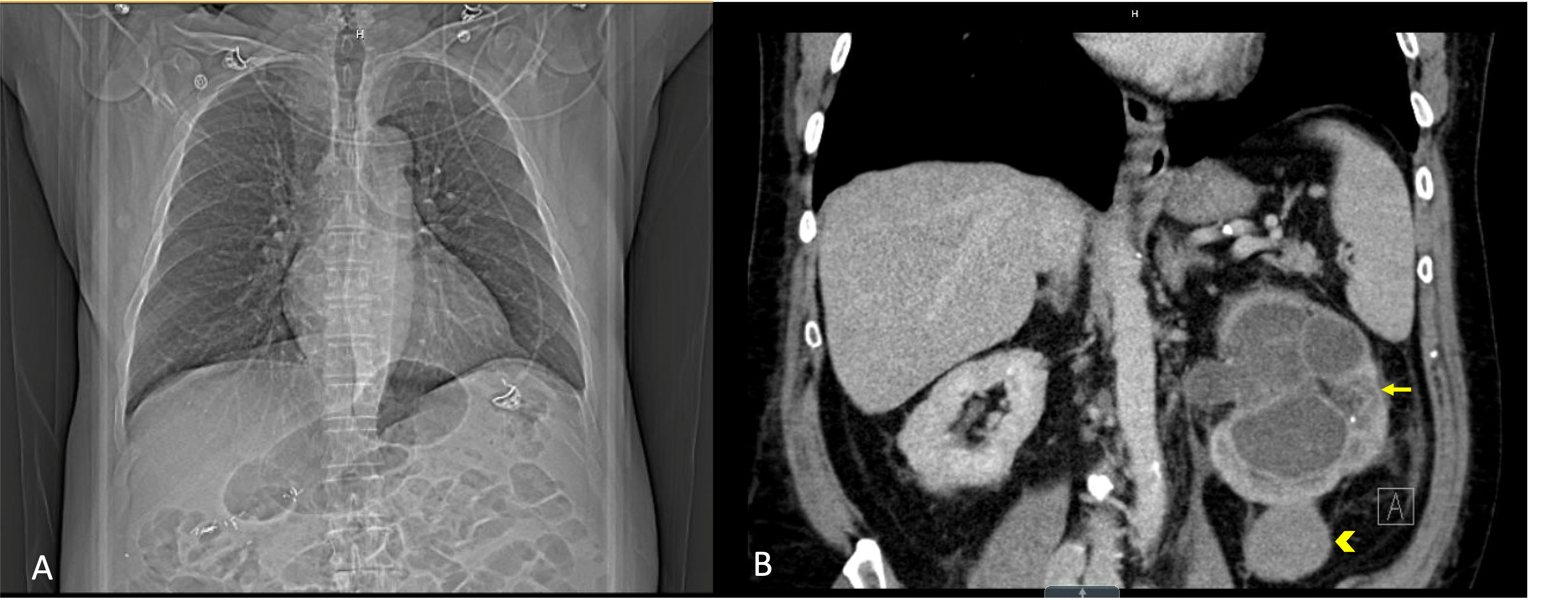
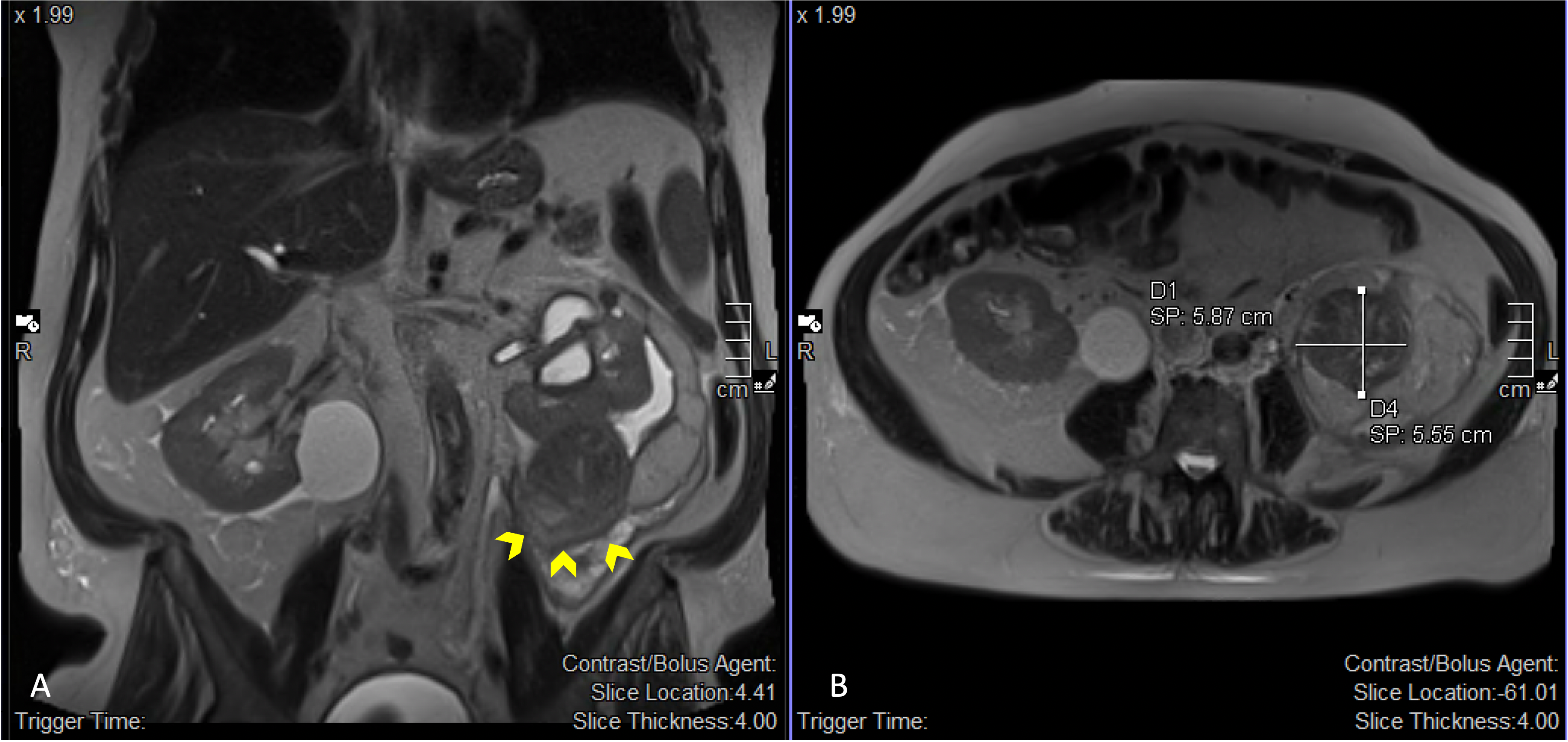
Case Presentation: A 76-year-old male with a history of allergic rhinitis presented to the hospital with four weeks of persistent dry cough. His cough is exacerbated by mild exertional activities and occurs at all hours. He had no nasal congestion, sore throat, hoarseness, hemoptysis, dyspnea, dysphagia, heartburn, or recent respiratory tract infection. He reported no new pets, mold exposures, or recent travel. He has a history of positive PPD tests; however, he was never treated for latent TB. He had tested negative for HIV previously and reported no high-risk sexual behaviors. He had a six-pack-year smoking history and quit >40 years ago. He had received antihistamines, cough suppressants, steroids, antibiotics, and changing ACE-i to ARB in the preceding weeks with no improvement. Besides his cough, he also reported night sweats and seven pounds of weight loss in the past month. The day before his presentation, he developed a fever of 102 F, which prompted his visit.On presentation, he was hemodynamically stable, saturating well on room air, but febrile at 104.5 F. Examination of his ear, nose, throat, and lung were unremarkable. No lymphadenopathy was noted. Laboratory studies revealed: a WBC of 14.5 and creatinine of 1.37 (baseline 0.99). A chest CT showed normal airways, lung parenchyma, and no lymphadenopathy. However, a 5 cm incidental mass was identified on the lower pole of the left kidney, causing severe hydronephrosis (figure 1). Urology was subsequently consulted for the hydronephrosis. He underwent a ureteroscopy, which revealed a narrowing of the left ureter. Pus drainage was noted after ureteral stenting. Urinalysis was consistent with UTI, and a diagnosis of pyelonephritis was made. His fevers resolved after stenting and initiation of ceftriaxone; however, his cough persisted. Subsequent MRI of the abdomen revealed a 5.7 cm complex mass on the lower pole of the left kidney, suspicious of neoplasm (figure 2). He later underwent a nephrectomy. Pathology revealed papillary renal cell carcinoma, grade 2, with pathologic stage pT1B. After the procedure, his cough resolved and has not recurred at the four-year follow-up.
Discussion: Many cases of renal cell carcinoma (RCC) are asymptomatic, often identified incidentally during the workup of another clinical issue. Less than 10% of patients present with classic flank pain, hematuria, and palpable abdominal mass. Persistent cough has been described as a rare paraneoplastic manifestation of renal cell carcinoma (RCC). A paraneoplastic cause for this phenomenon has been proposed based on observations that cough completely resolves following tumor resection or embolization and recurs in cases of cancer recurrence. Proposed mechanisms include tumor cell secretion of IL-6, bradykinin, or prostaglandins; however, no specific substance has been confirmed as the cause.
Conclusions: The case illustrates an uncommon but important cause of cough from an extrapulmonary source. The resolution of the cough following nephrectomy supports the previously documented paraneoplastic manifestation of RCC. When evaluating patients with a persistent cough, it is important to consider an extrapulmonary etiology, especially after common causes have been excluded.