Background: Pharmacist-led peri-discharge interventions reduce adverse drug events. However, evidence is lacking as to whether there is a business case to fund these non-billable interventions. To test whether such interventions could drive reductions in post-discharge health care utilization to help build a business case, we conducted a pragmatic randomized controlled trial (RCT).
Methods: The PHARMacist Discharge Care (PHARM-DC) intervention includes comprehensive medication review, communication with providers, addressing medication adherence and access, motivational interviewing, discharge medication reconciliation, and patient education around the time of discharge and via a post-discharge phone call. We implemented PHARM-DC at two large academic medical centers. A “best possible medication history” and admission medication reconciliation were provided for patients in both arms. Inclusion criteria were admission to a medical ward, age >55, medication complexity at admission (≥10 chronic prescription medications or ≥3 high-risk medications: anticoagulants, antiplatelets, insulin, and oral hypoglycemics), and expected discharge to home. Exclusion criteria included study enrollment in the prior year or planned receipt of similar interventions. The primary outcome was unplanned all-hospital acute care utilization within 30 days of hospital discharge, including emergency department visits, observation stays, and readmissions, based on Medicare claims data. We sought to randomize 9776 patients to achieve 80% power to detect an absolute reduction of 2.5% from an estimated baseline utilization of 27.5%. Proportions in each arm were compared using z-scores.
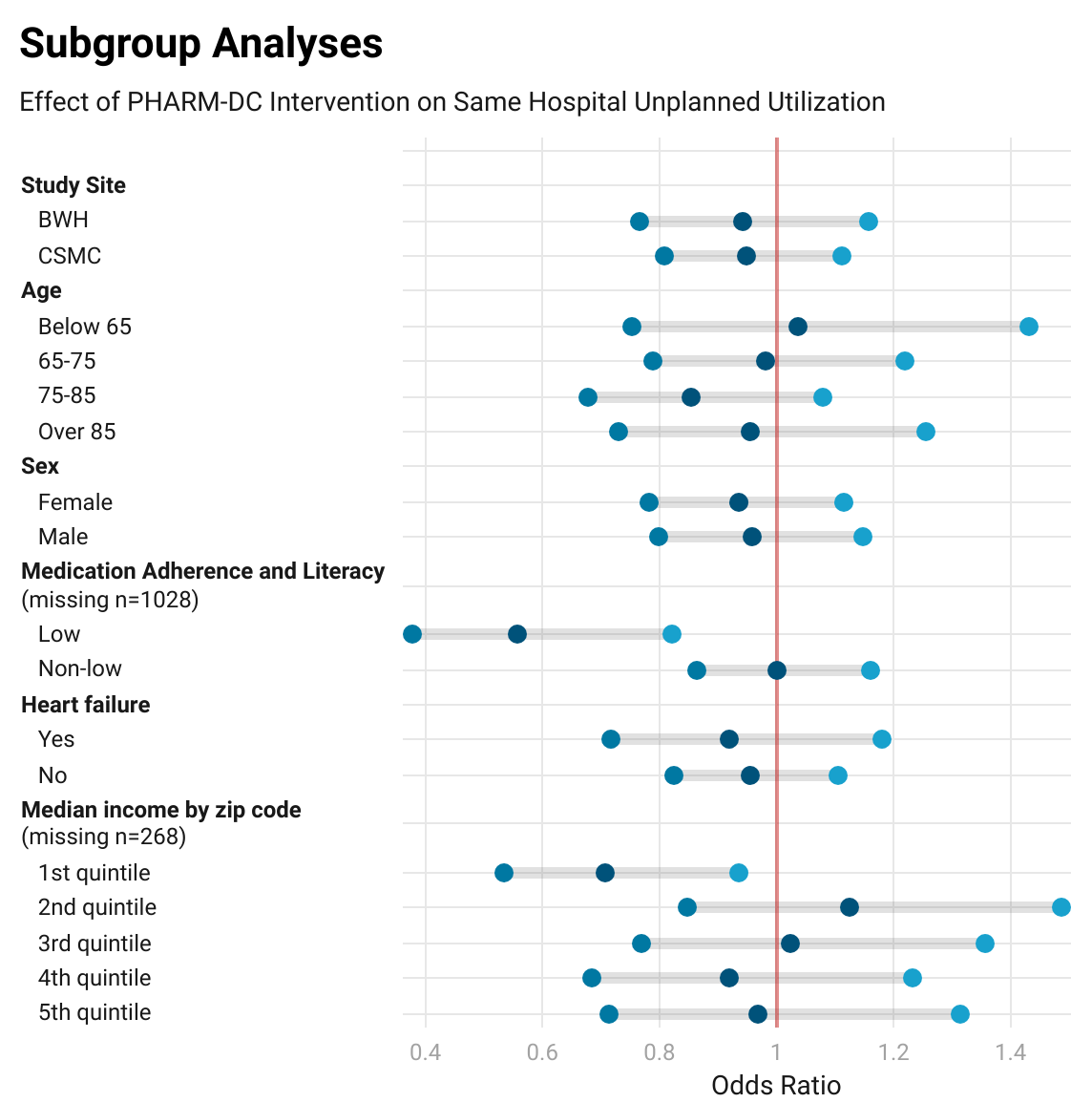
Results: We randomized 6478 eligible patients (3215 usual care, 3213 PHARM-DC, 50 lost to follow-up). Medicare claims data were available for 4602 patients. The COVID-19 pandemic, staffing shortages, and availability of eligible patients limited enrollment. The arms were well balanced in all measured characteristics except for the medication adherence and literacy (MedAL) score due to additional time for assessment among intervention patients. The number of patients with any unplanned all-hospital acute care utilization was 556 in the usual care arm (24.0%) versus 514 in the PHARM-DC arm (22.5%), an absolute reduction of 1.56% (95% CI -0.88, +04.00, p=0.21). In a priori-specified subgroup analyses of same-hospital unplanned utilization (Figure 1), patients with low MedAL scores had a 10.2% absolute reduction in utilization (95% CI 3.3%, 17.1%, p=0.003), with significant effect modification (p=0.006 for interaction between trial arm and low MedAL score).
Conclusions: In this RCT, one of the largest of its kind, a pharmacist-led peri-discharge medication management intervention did not significantly decrease all-hospital unplanned acute care utilization at two large academic centers when added to robust admission medication reconciliation programs. However, a significant reduction in utilization occurred in patients who screened positive for low medication adherence and literacy. Provider organizations seeking to improve patient outcomes and reduce avoidable utilization after hospital discharge should strongly consider adopting pharmacist-led transitions of care interventions for elderly patients with polypharmacy and low health literacy. Such interventions may offer financial returns to provider organizations under capitated, accountable care, and bundled payment models.