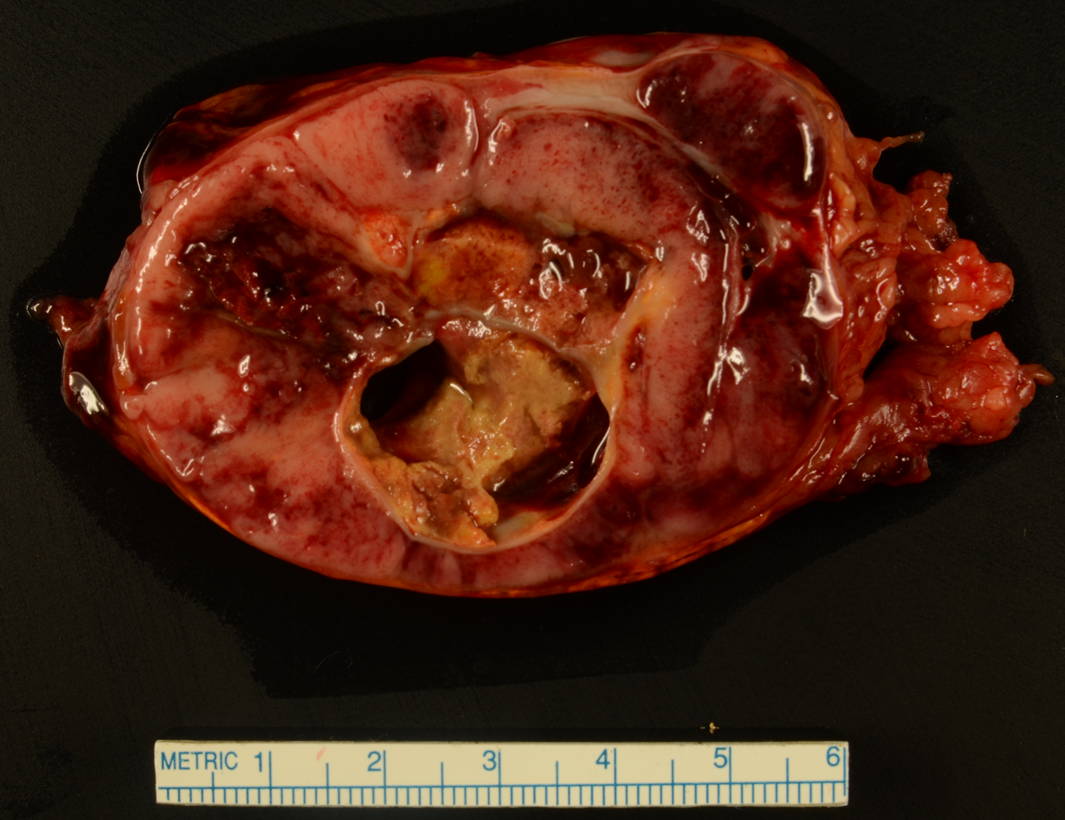
Case Presentation: 52-year-old female without significant history presented with 3 days of fever, sweating, and epigastric pain. BP 190/100 with heart rate of 86. Afebrile. Exam remarkable for mild abdominal tenderness. Laboratory testing demonstrated WBCs 27.3, lactate 4.8, troponin T 0.69, and NT pro-BNP 20,800. EKG showed sinus rhythm with nonspecific T wave changes. Negative abdominal ultrasound. Echocardiogram revealed EF 31% with regional wall motion abnormalities and grade 3/4 diastolic dysfunction. Coronary angiography revealed nonobstructive atherosclerosis with LVEDP of 32 mmHg. She subsequently became increasingly hypertensive and tachycardic and was given IV metoprolol, resulting in flash pulmonary edema requiring intubation. Abdominal CT revealed a hemorrhagic adrenal mass concerning for pheochromocytoma. Urine metanephrine and normetanephrine levels were elevated 70x and 20x upper reference limits, respectively. Pulmonary artery catheter demonstrated normotensive cardiogenic shock, so clevidipine and milrinone were initiated. Phenoxybenzamine, propranolol, and metyrosine were subsequently started prior to elective surgical resection of the mass three weeks later, with pathology confirming pheochromocytoma. EF recovered to 55%.
Discussion: Pheochromocytoma is a rare catecholamine-secreting tumor of the adrenal medulla managed by adrenergic blockade and resection. Critical care management is challenging, as in this patient presenting in extremis with catecholamine-induced cardiomyopathy, hypertensive emergency, and normotensive cardiogenic shock. Special considerations include antihypertensive medication selection, rapid diagnostic assessment, preoperative optimization, and surgical timing.
Conclusions: Pheochromocytoma is a rarely identified cause of acute cardiovascular instability. Pheochromocytoma should be considered in patients presenting with symptoms atypical for ACS. Carefully select antihypertensive agents when treating hypertension and tachycardia as β blockers can worsen patients with pheo. Catecholamine-induced cardiomyopathy from pheo is a rare, sometimes reversible, cause of heart failure; consider in the absence of typical risk factors.