Background: Point-of-Care Ultrasound (POCUS) training for hospitalists is important for direct patient care, supervision of Internal Medicine residents, and collaboration with Emergency Department and ICU providers. Current opportunities for POCUS training employ the I-AIM framework which structures learning objectives around indications, acquisition, image interpretation, and medical decision making. Unfortunately, learning image acquisition remains heavily time intensive creating barriers to POCUS training for many hospitalists.
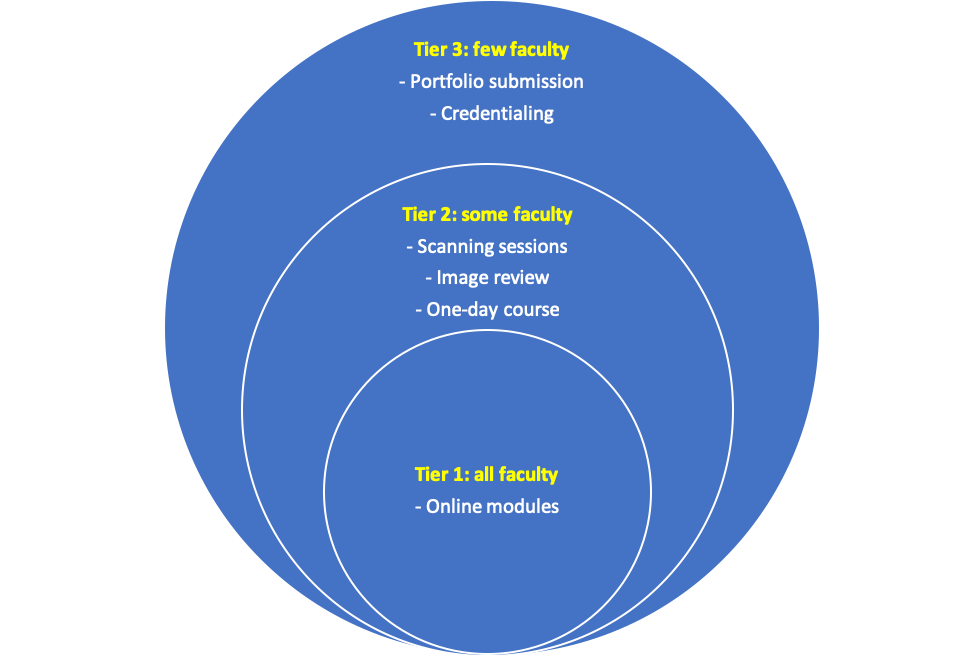
Purpose: Limited POCUS exposure is associated with poor knowledge and ability to safely supervise residents. To address this gap in a feasible way, we designed a tiered training pathway for our large hospitalist group. The goal of this tiered curriculum is to engage all hospitalists in basic knowledge and appropriate use (Tier 1); some hospitalists in hands-on image acquisition (Tier 2); and few hospitalists in quality assurance and formal credentialing (Tier 3). This approach of tiered training separates cognitive competency from image acquisition to decrease time commitment and increase engagement.
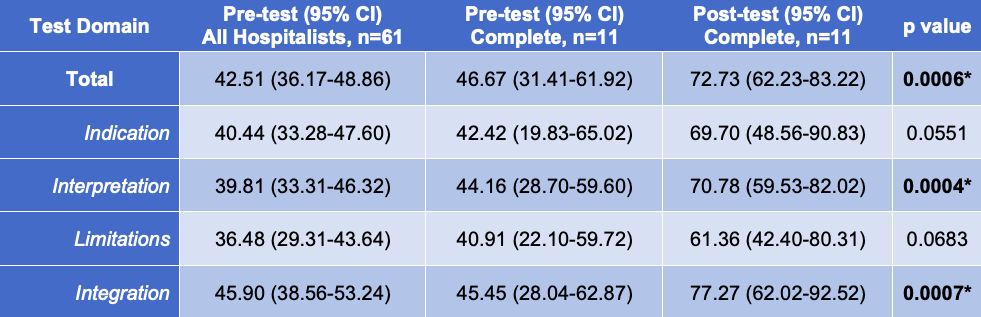
Description: Curricular Design:Figure 1 summarizes the tiered curriculum, which was incrementally introduced to our large hospitalist group over ten months and fully deployed in August 2019.Tier 1 includes five core online modules (basic knowledge, inferior vena cava, lung, cardiac, and abdominal POCUS). Tier 2 includes monthly image review sessions, supervised scanning sessions, and a single day course with both didactic and hands on elements. Tier 3 includes individual portfolio submission for credentialing. Curricular Assessment:Over the past 12 months, more than half of the hospitalists in our group (61/102) have engaged with at least one curricular element, with one-third of these being senior faculty (>10 years of practice). One-third (37/102) have viewed at least one online module, with twelve completing the entire cognitive curriculum. Nearly half have participated in at least one Tier 2 activity (48/102); and one-fifth have submitted images towards their portfolio (23/102). A knowledge test was e-mailed to all hospitalists preceding the start of the curriculum and to individual hospitalists upon their completion of the online modules. Survey results were aggregated, scored, and categorized based on the I-AIM framework, then analyzed using STATA 16. Pre and post-test results for those who completed the cognitive curriculum were compared using paired t-tests with p <0.05 considered significant. Completion of the online modules resulted in improved knowledge in every domain, with significant improvement noted in total score, image interpretation, and clinical integration (Table 1).
Conclusions: Our results demonstrate that a tiered training program for hospitalists can achieve two critical goals. First, structuring a training program to engage hospitalists with POCUS within their limitations encourages participation. Second, a cognitive-based curriculum can significantly increase hospitalists’ knowledge apart from gaining image acquisition skills. This is critical to safer supervision of residents using POCUS and improved collaboration with Emergency Medicine and ICU providers.