Background: Routine transfusion of platelets and Fresh Frozen Plasma (FFP) prior to paracentesis is among the “things we do for no reason”, as recommended against by the American Association of Liver Disease and American Gastroenterology Association in patients with platelets over 20,000. We hypothesize that a Medicine Procedure Service (MPS), which has adopted this recommendation for patients with cirrhosis (i.e., no strict cutoff for platelet or INR prior to paracentesis) into standard protocol may lead to lower rates of pre-procedure transfusion without an increase in post-procedural bleeding.
Methods: We conducted a retrospective cohort study of patients hospitalized at a tertiary academic medical center who underwent paracentesis between July 1, 2021 (MPS inception) and July 31, 2023. We collected electronic medical record data on frequency of pre-procedural (i.e., within 24 hours prior to paracentesis) and post-procedural (i.e., within 24 hours after paracentesis) blood products along with patient characteristics, pre-procedural laboratory parameters, and bleeding events. We compared pre-procedure blood product utilization between MPS and non-MPS performed paracentesis. As a safety outcome, we compared bleeding events, defined as either documented post-procedure bleeding or receipt of post-procedure blood transfusion, between MPS and non-MPS paracentesis.
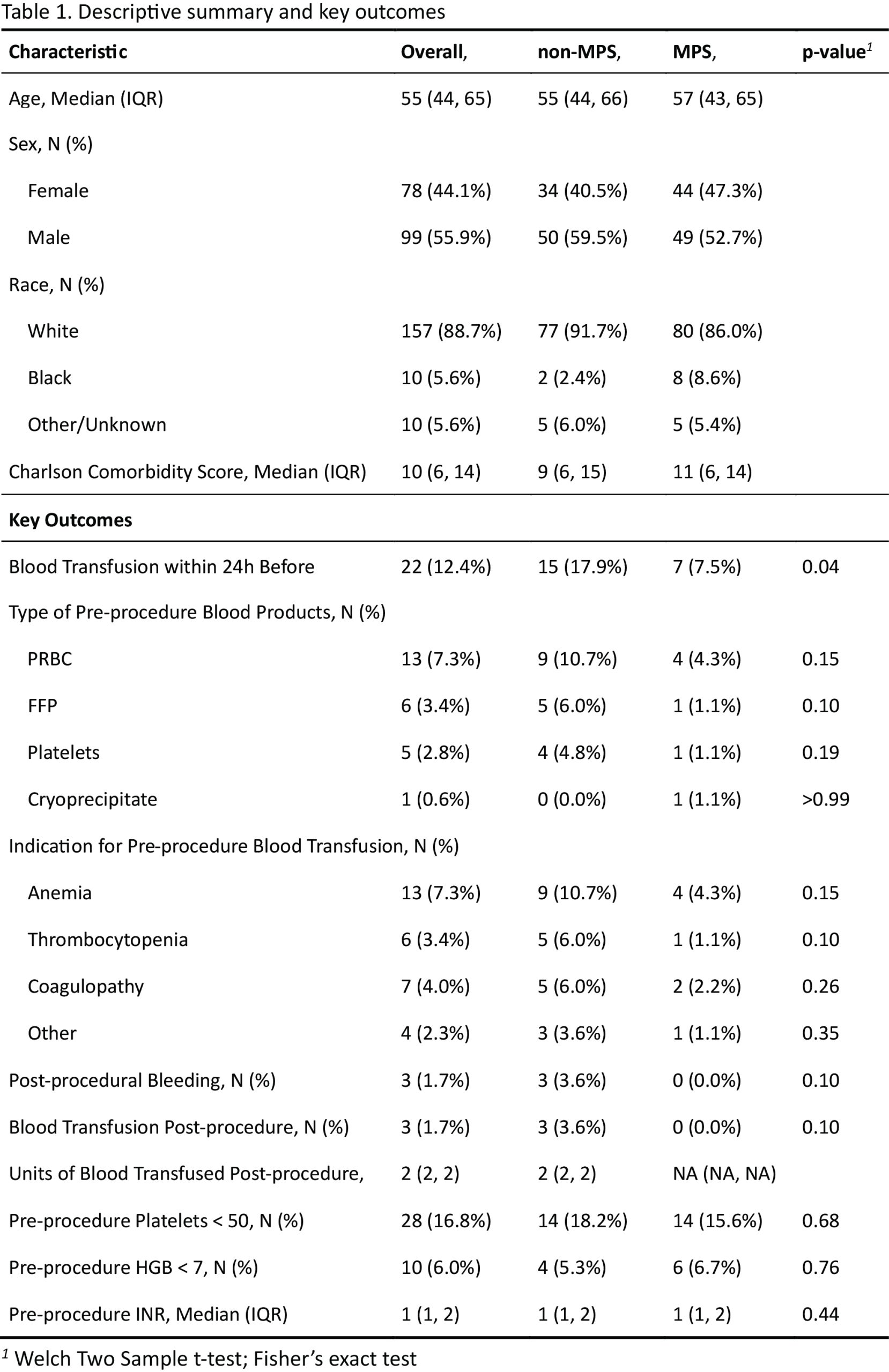
Results: Of 177 paracenteses performed during the study period, 93 (52.5%) were performed by MPS and 84 (47.5%) by non-MPS services. MPS and non-MPS cohorts had similar age and Charlson Co-morbidity Scores (Table 1). The proportion of patients with pre-procedural platelet count less than 50, hemoglobin less than 7, and median INR were similar between the two cohorts. Overall, pre-procedure blood product transfusion occurred in 22 (12.4%) of cases. A lower proportion of patients in the MPS cohort received pre-procedure blood products compared to the non-MPS group (17.9% vs 7.5%, p=.04). Three post-procedural bleeding outcomes were captured, all in the non-MPS cohort, (p=.10).
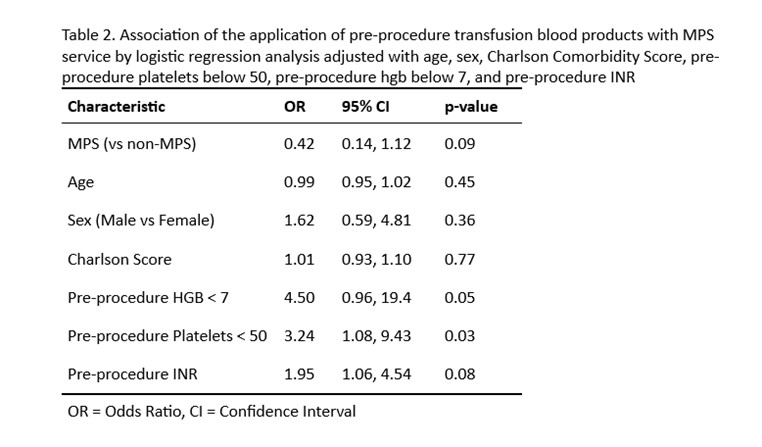
Conclusions: Our analysis found patients undergoing paracentesis by MPS less frequently received pre-procedure blood products than patients undergoing paracentesis by other services, despite similar age, comorbidities, and pre-procedure platelet, hemoglobin, and INR. There was no increase in post-procedure bleeding. These findings support the role of a Medical Procedure Service in safely implementing evidence-based peri-procedure blood product stewardship practices.