Background: Inter-hospital transfer (IHT, patient transfers between acute care hospitals) is common among hospitalized medical patients (1). However, few data describe which patients may be exposed to the risks of discontinuity of care from IHT without clear benefit (i.e., undergo potentially inappropriate IHT).
Methods: The POINT Study, “Identification and Prevention of Potentially Inappropriate Inter-Hospital Transfers” (AHRQ-R01HS028621) aims to define and evaluate the prevalence and impact of potentially inappropriate IHT across a nationally representative sample of 16 tertiary/quaternary care referral hospitals. We first carried out focus groups of key stakeholders to generate a consensus definition of potentially inappropriate IHT, translated the definition into an adjudication tool, and conducted rigorous adjudication training across sites (2). Each site then conducted retrospective chart reviews on 100 randomly selected medical patients that underwent an IHT between March 2022 – August 2023, rating each on level of appropriateness using a 6-point scale (highly appropriate to highly inappropriate), and abstracting data on IHT processes and care after transfer. Reviews were conducted by 2 independent adjudicators who then met to come to consensus. Level of appropriateness was dichotomized and analyzed descriptively to report overall prevalence of potentially inappropriate IHT and evaluate explanatory reasons (e.g., could have been served by an alternative care modality). We combined adjudicated data with administrative data from Vizient Clinical Data Base to conduct multivariable logistic regression analysis, clustered by site, to identify patient-, hospital-, and transfer process-related predictors of potentially inappropriate IHT, correcting for multiple testing. Here we report on the results from 12 of 16 sites.
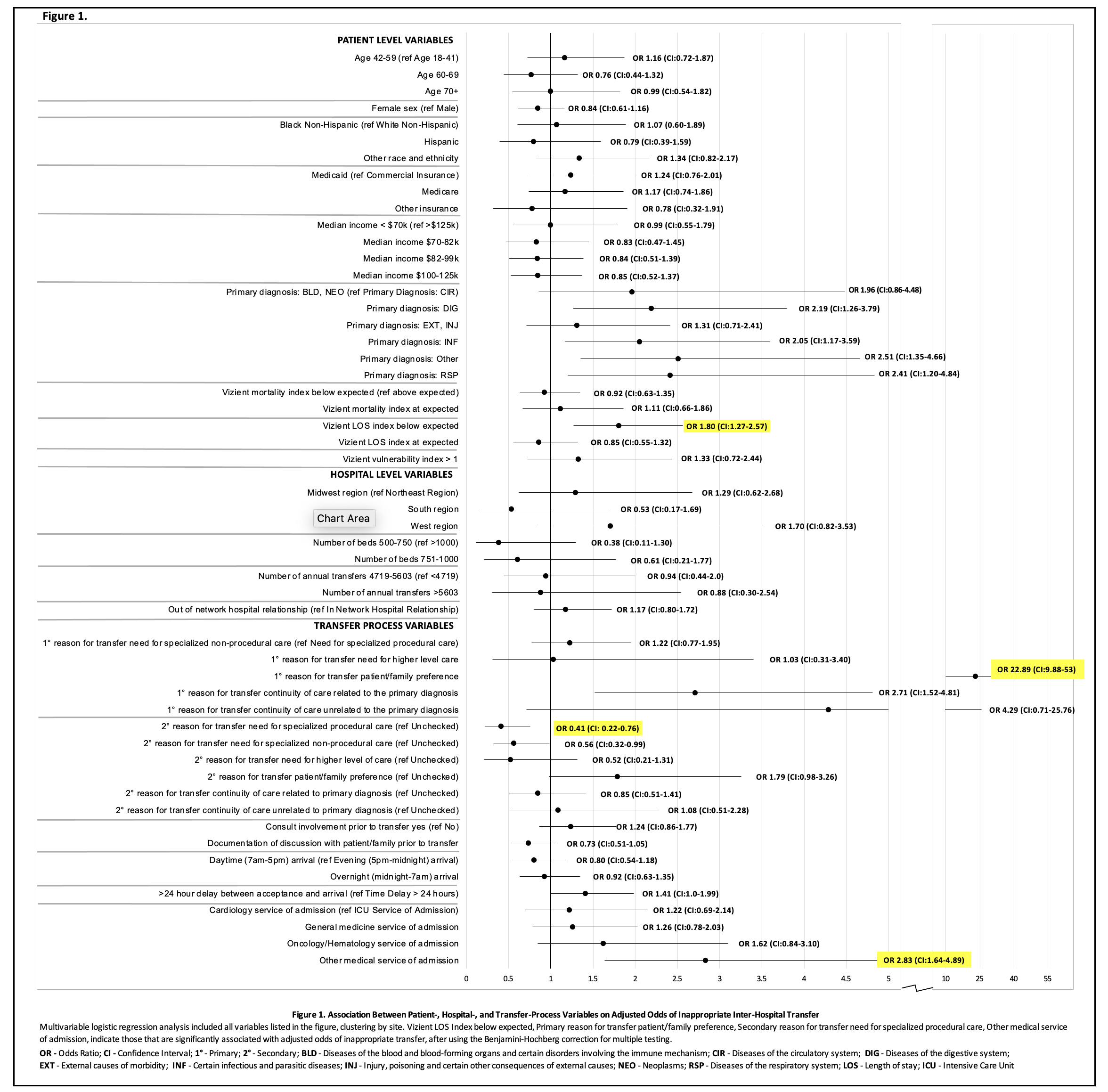
Results: Characteristics of the included patients are shown in Table 1. Among 1200 patient transfers, 279 (23%) were deemed inappropriate, with site-specific prevalence ranging between 10-46%. Among inappropriate IHT patients, 248 (89%) could have been served by an alternative to transfer. Tele-consult was the most commonly selected alternative, in 210 (75%) of inappropriate IHTs, but was available in only 90 transfers (32%). In 181 (65%) patients, care needs could have been met at the transferring hospital, and 19 (7%) did not have urgency to their care need (i.e., could have had outpatient management). In multivariable analysis, primary reason for transfer of ‘patient/family preference’, lower patient length of stay acuity index, and admission to a specialty medical service were associated with increased adjusted odds of inappropriate IHT, while secondary reason for transfer of ‘need for specialized procedural care’ was associated with decreased adjusted odds of inappropriate IHT (Figure 1).
Conclusions: In this national evaluation of 1200 transferred medical patients, we found that nearly one quarter (23%) were potentially inappropriate, e.g., could have been served by another modality of care. Tele-consults were considered a potentially useful solution but were rarely available in current practice. We further identified several notable predictors of inappropriate transfer including reason for transfer, patient illness severity, and service of admission. While patient preferences will need to be incorporated into future changes to IHT, our research suggests several targets for system-based approaches to reduce inappropriate IHT.
.jpg)