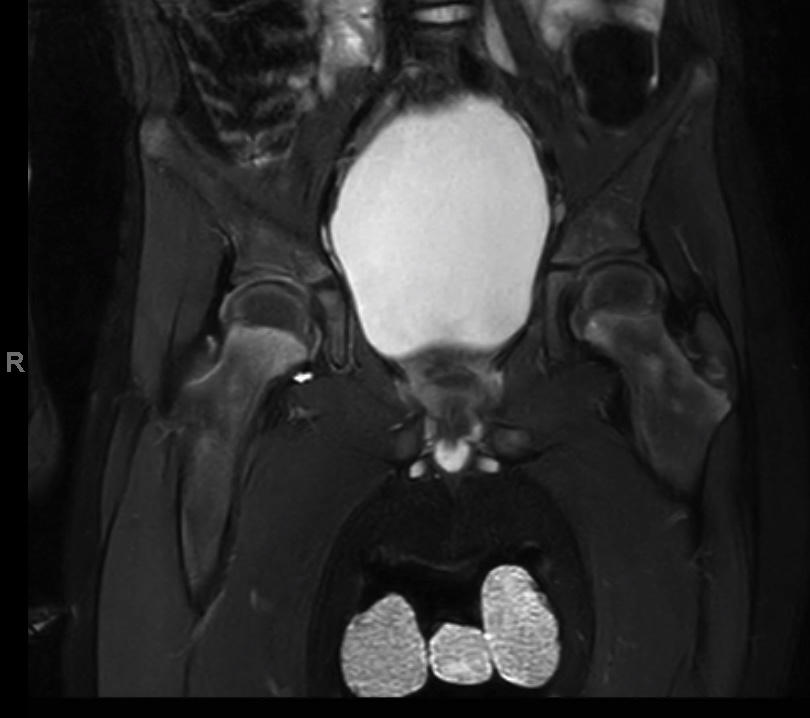
Case Presentation: A four-year-old boy with a history of non-verbal autism was admitted with one week of progressive bilateral lower extremity weakness and pain. Past history was significant for a diarrheal illness 1 month prior. Exam findings included poor dental hygiene, gingival hypertrophy with ecchymosis and bleeding, intact reflexes and 3/5 lower extremity strength. Labs (CBC, CMP, CRP, ESR) and imaging (MRI spine, US hips and X-ray hips) were normal. Cerebral spinal fluid was within normal limits and without albuminocytologic dissociation. Neurology was consulted and patient was diagnosed with Guillain-Barre syndrome based on symptomatology and expert consensus; he received IVIG with modest improvement in extremity strength and was discharged. He was readmitted 2 days later with worsening pain and inability to bear weight. Exam showed agitation during manipulation of hip and knee joints and worsening gingivitis. Bilateral hip MRI showed abnormal signal enhancement in pelvic metaphyseal zones suggestive of scurvy. History revealed a restrictive diet consisting mainly of blue Gatorade with minimal fruit and vegetable intake. Serum Vit C level was undetectable and he was started on IV ascorbic acid. His symptoms improved rapidly, and he was discharged 4 days later on Vit C supplementation with PCP & nutrition follow up.
Discussion: Scurvy is a condition caused by severe Vit C deficiency. Vit C, found in fresh fruits and vegetables, is an essential micronutrient required for the biosynthesis of collagen, L-carnitine, and neurotransmitters; it aids in iron absorption, folate utilization, and is a potent antioxidant(1,2). Humans are unable to independently synthesize Vitamin C and depend on intake to maintain normal levels. Children at high risk for Vitamin C deficiency include those with oral aversion, cerebral palsy, and developmental disorders, or those who suffer from parental neglect(3). Infants who are exclusively fed evaporated or boiled milk, which destroys ascorbic acid, are also at increased risk of developing scurvy(4). The clinical manifestations of scurvy arise from defects in collagen synthesis and weakening of the skeleton and blood vessels. Prolonged deficiency can result in lethargy, failure to thrive, anorexia, gingival hyperplasia and bleeding, cutaneous findings such as perifollicular petechiae and abnormal bone and cartilage formation(5). Characteristic imaging findings include ‘scurvy lines’ which represent decreased cartilage proliferation with normal mineralization(6,7). Difficulty with ambulation is the most common presentation in children(8,9).Our four-year-old boy had symptoms of musculoskeletal pain, gingival hyperplasia and lower extremity weakness. His developmental disorder was associated with limited food intake and subsequent chronic Vitamin C deficiency. His presentation represented a diagnostic challenge given the broad differential of inability to walk and the preceding diarrheal illness persuaded providers to consider the more common diagnosis of GBS during his initial admission.
Conclusions: Given its rarity in the developed world, Vitamin C deficiency is often overlooked and patients undergo an extensive workup which delays diagnosis and treatment. It is imperative to have a high index of suspicion when encountering at risk patients and obtain a thorough dietary history(10). Treatment with Vitamin C is effective with quick resolution in symptoms. Referral to nutritional support to improve oral intake is crucial for long-term management.