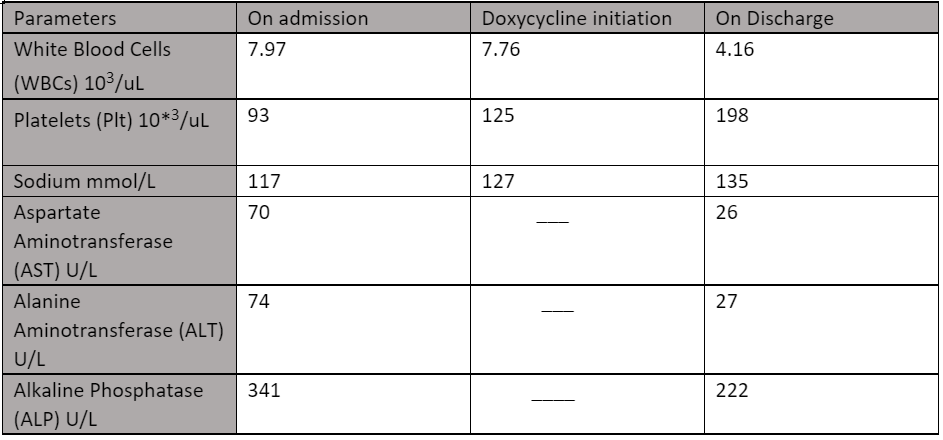
Case Presentation: A 54-year-old man presented with fever and malaise for two weeks associated with chills, non-bloody diarrhea, and unintentional weight loss of 8 lbs. He tested positive for influenza-A two weeks prior to presentation and was started on Oseltamivir by his primary care physician, without symptomatic improvement. There was no recent history of sick contacts, however, the patient reported having close contact with stray cats and dogs. On physical examination, temperature was 102.1 °F, rest of the vital signs and examination were normal. Initial laboratory workup showed hyponatremia – sodium 117 mEq/L, elevated AST 70 U/L, ALT 74 U/L, alkaline phosphatase 341 U/L, and thrombocytopenia with a platelet count of 93 x 103 /uL. The gastrointestinal panel was negative for common bacterial and viral causes of acute diarrhea. An ultrasound of abdomen showed liver with heterogeneous echogenicity, which could result from fatty liver infiltration, hepatitis or cirrhosis, however the patient had a normal coagulation profile, and CT scan abdomen and had no stigmata of liver cirrhosis. Based upon the clinical presentation and laboratory findings, suspicion of Murine typhus was high, especially given the endemic nature of the disease in the Rio Grande Valley and patient’s exposure to possible vectors/reservoirs. The patient was started empirically on doxycycline on day 2 of admission, Weil-Felix test was positive (Proteus OX-19 antibody positive 1:320) and Typhus IFA (Immunofluorescence) were positive with IgM titer 1:256 and IgG titer 1:64 indicating a diagnosis of Murine typhus. The patient showed significant clinical improvement with doxycycline therapy and was discharged home to complete the antibiotic regimen.
Discussion: The etiologic agent of Murine typhus is Rickettsia typhi, an aerobic, obligate intracellular, gram-negative bacterium (1) . Domestic cats, rats and opossums are common reservoirs, while rat fleas and cat fleas are common vectors. Common modes of transmission include bacteria in flea feces entering through the flea bite site or a different area of skin disruption or are introduced into the conjunctiva due to eye rubbing. Inhalation of dried cat flea feces is also a possible mode of transmission (2,3). According to Texas department of State Health Services data from 2008-2019, a total of 1534 cases were reported in Rio Grande Valley with the highest number of cases reported in Hidalgo County (1053), followed by 388 cases in Cameron County and 54 and 39 cases in Starr and Willacy counties, respectively (4). Physicians should have a high suspicion of Flea-borne (Murine) typhus in patients presenting with fever, elevated transaminases, and thrombocytopenia, especially in endemic typhus areas such as Rio Grande Valley. Confirmation of the diagnosis can be challenging especially when resources are limited, but physicians should have a low threshold for initiating empiric doxycycline therapy. Moreover, it is imperative to educate the patients and their family members about flea-borne typhus and preventive strategies recommended by CDC (Centers for Disease Control).
Conclusions: Murine Typhus should be suspected in patients with fever, thrombocytopenia, and elevated transaminases, especially in endemic areas such as Texas and California. Prompt treatment with Doxycycline can prevent the progression to life threatening illness and shorten the disease course (5).