Background: Even after successful treatment, many patients with tuberculosis (TB) suffer from post-TB sequelae. These may be structural complications (such as bronchiectasis, broncholithiasis, residual cavitation, COPD), infectious complications (such as COPD exacerbations, Aspergillus fumigatus infections, non-tubercular mycobacterial infections, pneumonia), or psychosocial morbidities (such as anxiety, depression, financial burden).[1] The impact of post-TB sequelae is not only restricted to clinical outcomes but also includes the Health-Related Quality of Life (QoL) and psycho-social well-being.
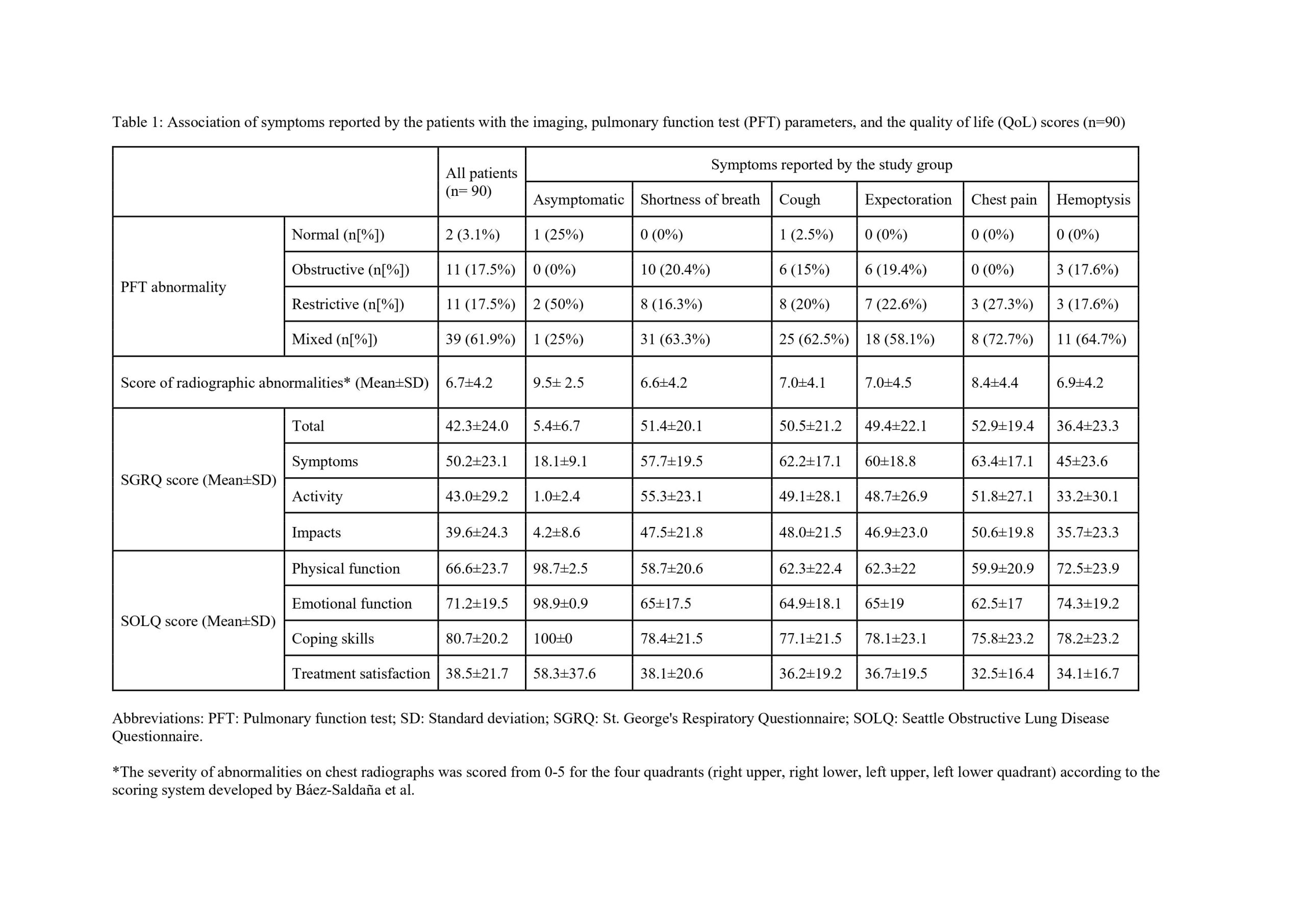
Methods: This was a cross-sectional single center study performed in the chest clinic of a tertiary care academic medical center in northern India over a period of six months. Patients >18 years of age with a history of pulmonary TB whose symptoms could not be explained by a concomitant disease were included in the study. Clinical history was elicited by interviews. PFT and chest radiographs were also recorded. The severity of abnormalities on chest radiographs was scored from 0-5 for the four quadrants (right upper, right lower, left upper, left lower quadrant) according to the scoring system developed by Báez-Saldaña et al.[2] The severity of dyspnea was evaluated using mMRC grading. QoL assessment was done using two standardized questionnaires- St. George’s Respiratory Questionnaire (SGRQ) and Seattle Obstructive Lung Disease Questionnaire (SOLQ).
Results: A total of 90 participants (mean age 40.4±11.6 years; 60 [66.7%] males) were recruited in the study. Overall, 84 (93.3%) patients were currently symptomatic (table 1), with the most common symptom being shortness of breath (67 [74.4%]). Most patients (61 [96.8%]) had abnormal PFTs, out of which majority (39 [61.9%]) had a mixed ventilatory defect. Chest radiographic abnormalities were present in 60 (92.3%) patients with the mean chest radiographic score being 6.7±4.2. On assessment of QoL by SGRQ, patients with chest pain (mean total score 52.9±19.4) had the most affected QoL, followed closely by shortness of breath (mean total score 51.4±20.1). Across the four domains of SOLQ, patients with chest pain (emotional function domain, mean score 62.5±17; coping domain, mean score 75.8±23; treatment satisfaction domain, mean score 32.5±16.4) and shortness of breath (physical function domain, mean score 58.7±20.6) had the most affected QoL. Significant negative correlation was seen between the domains of SGRQ as compared to SOLQ (p< 0.001).
Conclusions: Even after successful completion of treatment for pulmonary TB, most patients continued to have persistent respiratory symptoms, radiographic and PFT abnormalities. Further, these post-TB sequelae are accompanied by significant impairment in QoL in these patients, especially in patients with chest pain and shortness of breath. Given the risk of a poor QoL, patients suspected to have post-TB sequelae should be referred to a higher center for appropriate care.