Background: Unplanned hospital readmissions are a burden on patients and cost taxpayers tens of billions of dollars each year in the United States1. Multi-component interventions have been the most effective at readmission reduction.2. But with hospital resources spread thin, it may not be necessary or even feasible to provide a multicomponent intervention for all discharging patients. Demographic and chart data have been used in prediction models to identify at-risk patients for these interventions. However, current prediction models fail to incorporate patient perceptions of their health, support, and readiness for discharge. To further refine and advance these models, patient-centric risk factors for readmission must be explored and identified.
Methods: Forty-nine patients enrolled by convenience sampling from two inpatient units at a large academic hospital were asked to fill out 19-item surveys inquiring about support at home, quality of care, and self-perceptions of health status. Patients were followed prospectively for any unplanned 30-day readmissions. Patient chart data and responses to survey items were analyzed to evaluate correlations with readmission rates. Since all variables in the data set were categorical in nature, Fisher’s exact test was used to test the association between readmission status and variables such as (stratified) age, gender, patient’s expected return date, discharge readiness, etc. Statistical software SAS (version 9.4) was used to perform the statistical analysis.
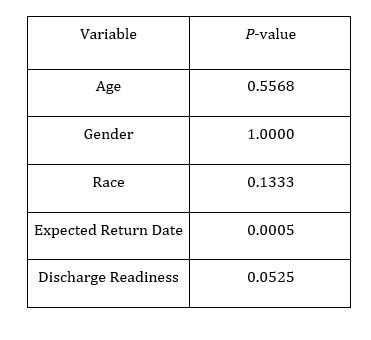
Results: In our final data set of size n = 49, we observed that 8 (16.33%) subjects were readmitted within 30 days of discharge from the hospital. Using Fisher’s exact test, we found that readmission status was significantly associated with patient’s expected date of readmission. We also observed a marginally significant association between readmission status and patient-reported discharge readiness. Based on the collected data, we do not have sufficient evidence to claim that readmission status is associated with age, gender, or race.
Conclusions: The preliminary data indicates that patients’ expected readmission date and their perceived readiness for discharge can help identify risk for readmission. This suggests that patients themselves can provide crucial information regarding their risk for readmission. Further study is thus needed to confirm these risk factors and incorporate them into prediction models for readmission.