Background: Venous thromboembolism (VTE) is a serious and all too frequent hospital complication, therefore assessing each patient’s individual risk of VTE is an important part of their care. Multiple models are available for risk assessment, however most not only include multiple data points requiring redundant entry, but can be labor intensive and time-consuming to complete on initial evaluation. Current guidelines recommend VTE prophylaxis be utilized based on the patient’s potential risk, with no prophylaxis being used in the low risk population. This recommendation has been further supported by recent studies showing the potentially deleterious effects of the overuse of prophylaxis. However due to the cumbersome nature of current manual risk assessment, many patients are placed on prophylaxis reflexively on admission, regardless of risk.
Purpose: The aim of our innovation is to develop a real-time, automated assessment of patient VTE risk based on elements that already exist in the electronic health record (EHR). The risk assessment would then be integrated into the physician workflow on admission to improve the appropriateness of VTE prophylaxis orders, and therein improving patient safety.
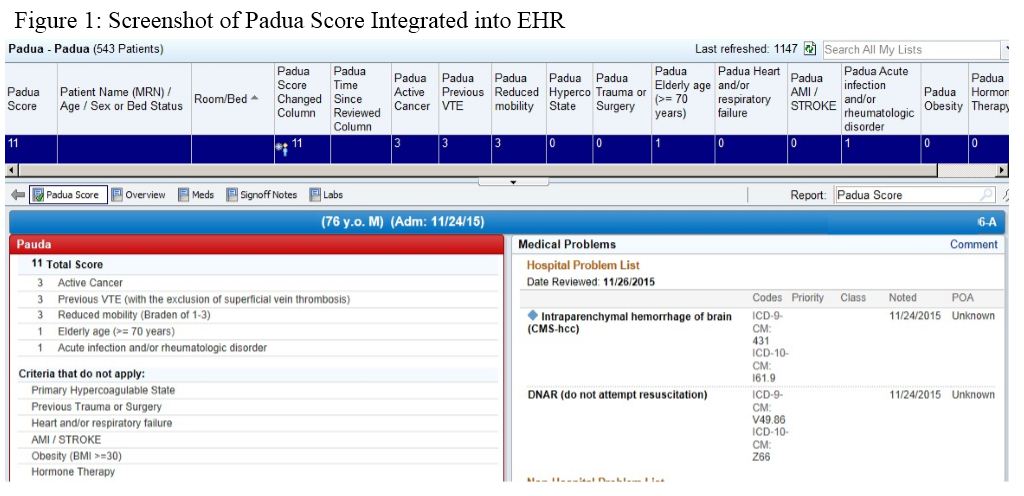
Description: A multi-disciplinary team of nurses, physicians, analytics personnel, and information technologists was formed to create, validate, and implement the risk assessment tool. The Padua score was chosen as the preferred risk assessment model based on its strong validity and relatively fewer data points required. Variables of the risk assessment tool are pulled directly from the patient’s already documented medical history and current problem list in the EHR, which requires utilization of problem-based charting within the EHR. There is no need for any additional data entry from the user other that normally required for documentation of the history and physical exam. Mobility, a relatively subjective element of the risk assessment model, is calculated by nursing documentation of the Braden score as a surrogate marker. Manual chart review is being completed to verify the automated data pull and to identify areas of improvement prior to it being operationalized. When the cumulative risk score is calculated, it is linked to a color code to clearly specify the patient’s relative risk of VTE (low, intermediate, or high). This risk score and stratification will be represented to the provider as they enter the chart in the form of an alert, with information detailing the guideline-based treatment recommendations for each stratum of risk. Once fully integrated into the EHR, the risk assessment will be implemented at all of our health system hospitals.
Conclusions: VTE risk assessment is an important aspect of patient care, but can be time consuming and is often overlooked. By employing an automated risk assessment tool, providers can more effectively prescribe appropriate levels of prophylaxis more efficiently. A multi-disciplinary team is an essential element of creating this tool, given the various levels of stakeholders related to direct patient care and maintenance of the EHR. Once fully implemented, we intend to track rates of guideline-based VTE prophylaxis use to determine the true effect size of the change and its impact on patient safety.