Background: Physical function (PF) impairment is a key determinant of hospital discharge disposition, yet real-time PF assessments remain underutilized in inpatient care. The Patient-Reported Outcomes Measurement Information System Physical Function 5-item tool (PROMIS PF5, or PF5) was embedded into the electronic health record (EHR) across 21 Kaiser Permanente Northern California (KPNC) hospitals to standardize PF assessment and integrate it into care. Here, we evaluated its utility in predicting discharge disposition (to home, home with home health services [home health], or to a skilled nursing facility [SNF]).
Methods: Our retrospective cohort study included inpatient and observation encounters from 21 KPNC hospitals (January 1, 2022, through March 31, 2024). PF5 data included patient-reported prior level of function (PLOF) and clinician-assessed current level of function (CLOF), updated daily. Gradient-boosted machine models predicted discharge disposition using demographic, clinical, and functional covariates. Model performance was evaluated across the first 7 days of hospitalization using area under the receiver operating characteristic curve (AUC), precision-recall AUC (prAUC), and number needed to evaluate (NNE), and were compared to models using manually entered expected discharge dispositions (EDD).
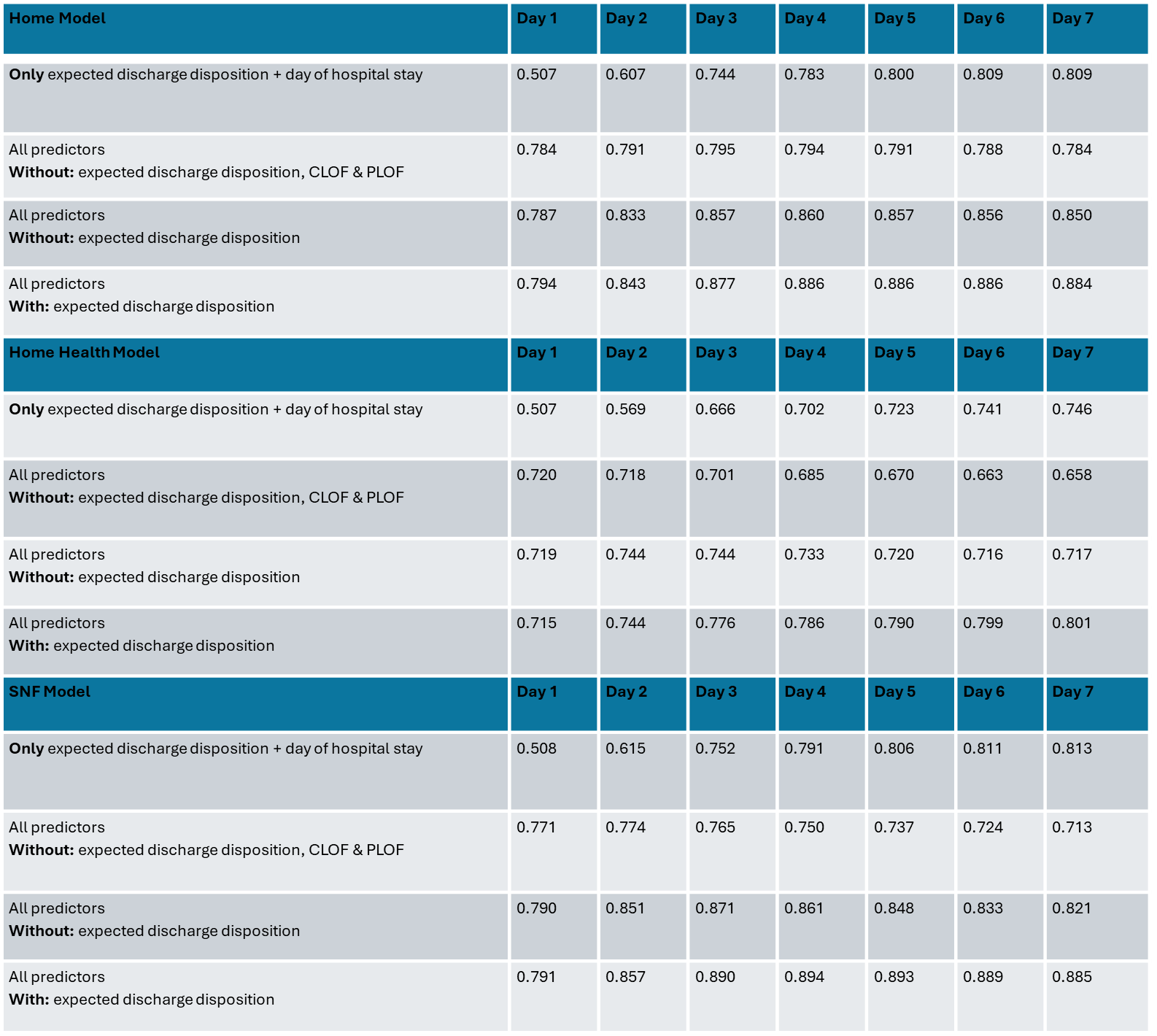
Results: PF5-based models outperformed manually entered EDD, especially early during hospitalization when EDD was often missing. Across 493,035 hospital encounters, PF5 – particularly CLOF – strongly predicted discharge disposition outcomes. For example, on day 3 of hospitalization, SNF discharge predictions using models with PF5 achieved an AUC of 0.89 (vs. 0.75 using EDD alone). CLOF was the most influential predictor across models. The NNE for SNF discharge improved from 4.0 (Day 1) to 1.4 (Day 7) at a sensitivity threshold of 60%. Models for home and home health disposition similarly showed improved accuracy with PF5.
Conclusions: Models incorporating physical function improved prediction of discharge disposition, significantly outperforming models using expected discharge disposition alone. Models incorporating PF data, including the PF5, can provide earlier, more accurate insights for discharge planning and support broader implementation of integrated functional assessment tools to optimize post-acute care transitions and hospital throughput.
.png)