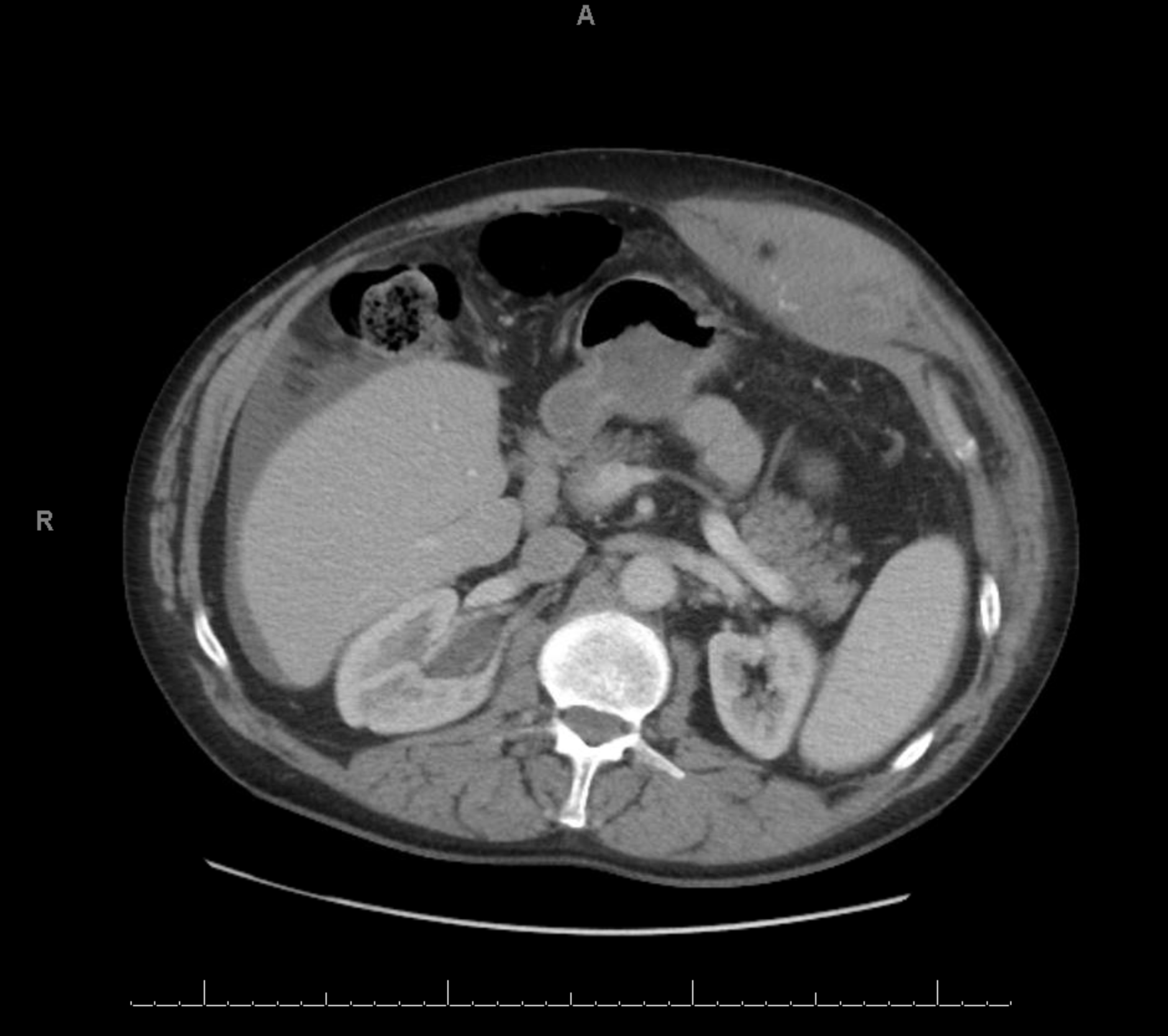
Case Presentation: 62-year-old male presenting to the hospital for left sided abdominal pain. His past medical history is significant for chronic obstructive pulmonary disease (COPD) requiring six liters of oxygen via nasal cannula daily, hypertension and hyperlipidemia. He states that he had a cough attack and then proceeded to have sudden onset of severe left sided abdominal pain. The pain was so severe that he decided to bring himself to the hospital. His vital signs on arrival unremarkable, with heart rate of 92 beats per minute and normal blood pressure. Physical examination of his abdomen showed abdominal distention with erythema, firm mass and tenderness to palpation localized in the left upper and lower quadrant. His laboratory examination showed a hemoglobin level of 11.5 gm/dL and a leukocytosis to 13.8. He had a computed tomography of the abdomen and pelvis done on admission to the hospital. It showed an acute rectus sheath hematoma within the superior aspect of the left rectus abdominis muscle belly with internal active hemorrhage and hematocrit effect. He did not report any recent trauma or a history of daily or recent anti-platelet or anticoagulation use. General surgery was consulted at this time but they did not recommend any acute surgical intervention or drainage. Throughout his five-day admission, his hemoglobin remained stable. His abdominal pain improved with oral analgesia with oxycodone. He was discharged home on an abdominal binder with close follow up with his primary care physician.
Discussion: Accumulation of blood due to a ruptured branch of the inferior epigastric artery within the rectus sheath leading to a rectus sheath hematoma (RHS) formation has been reported to be a rare finding, especially in a non-traumatic setting without an increased risk of bleeding. One of the most common causes of non-traumatic RSH formation has been seen in the setting of antithrombotic therapy. However, our patient denied any use of antithrombotic agents but his history COPD placed him at a higher risk for RSH formation. It typically presents with localized abdominal pain that can be misleading for other acute intra-abdominal pathologies. A high clinical suspicion with a through physical examination is key to diagnosing a patient with RSH. Some of the key physical examination findings include but not limited to Carnett’s sign, increased pain with abdominal muscle contraction, and Fothergill’s sign, abdominal wall mass does not cross midline, latter of which our patient presented with. Treatment for RSH can range anywhere from conservative treatment, as in our patient, to surgical treatment in severe cases that lead to rupture into the peritoneal cavity.
Conclusions: Rectus sheath hematoma (RSH) is a rare clinical and radiographic finding. It requires an astute physician to have high clinical suspicion with a thorough physical examination in the setting of acute abdominal pain, especially when considering non-traumatic etiologies for RSH.