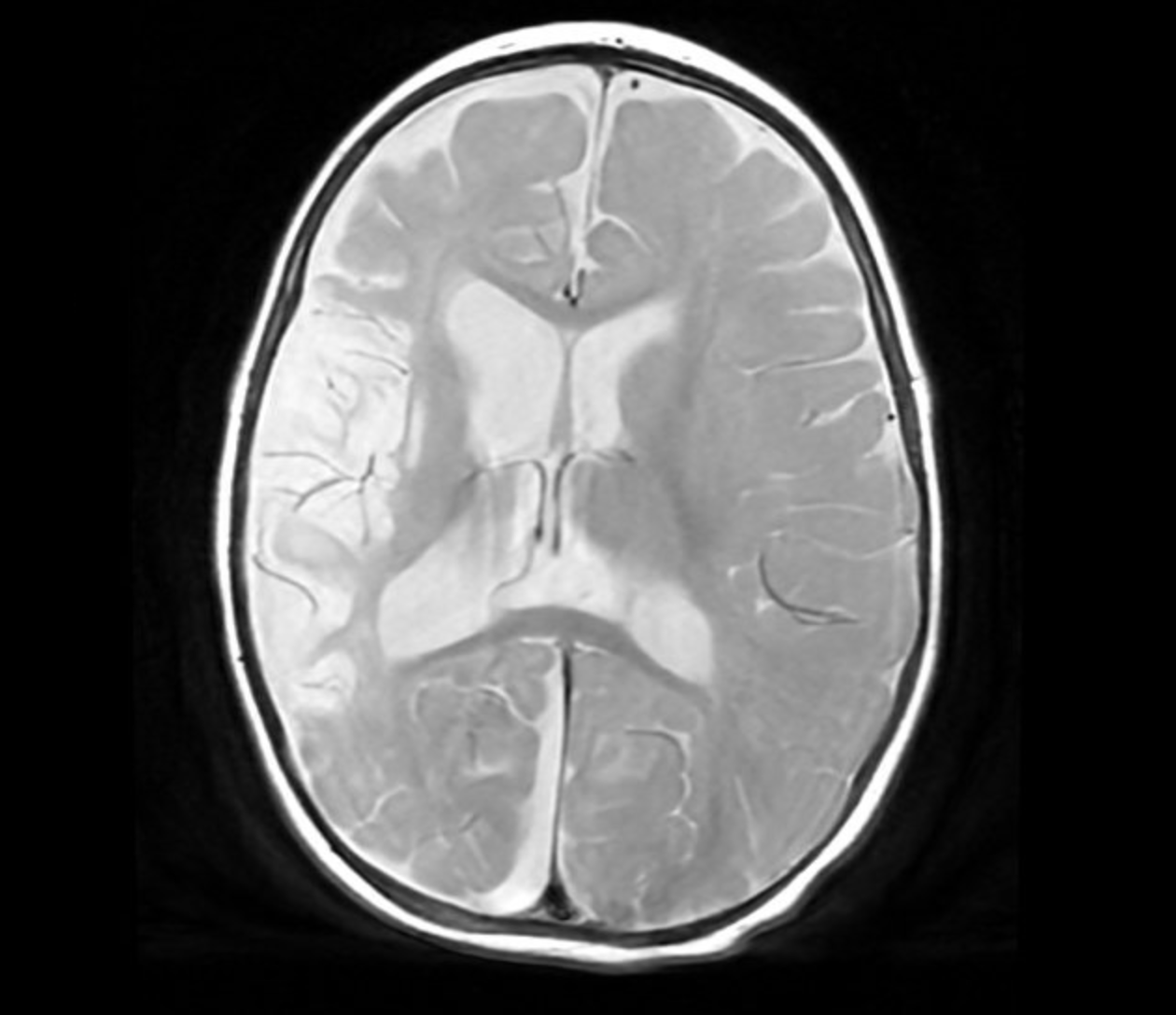
Case Presentation: A 4-month-old unvaccinated male, presented with left-sided weakness and decreased activity. Initial physical exam demonstrated right gaze deviation, left hemineglect, decreased left-sided movements, and absent left plantar reflex. Labs showed leukocytosis 22.8 K/uL, anemia 8.6gm/dL, and thrombocytosis 661K/uL. CT brain demonstrated intracerebral edema in the distribution of the right middle cerebral artery (MCA). MRI showed abnormality of the right internal carotid artery with narrowing beyond the terminus, and secondary changes of subacute infarct of right MCA. Ceftriaxone, Keppra, and Aspirin were started. Lumbar puncture performed; meningitis/encephalitis panel positive for Hemophilus influenza, complicated with right (MCA) stroke. Hematology/Oncology excluded thrombophilia. Audiology evaluation revealed reduced right ear responses and ABR confirmed sensorineural hearing loss on the right side. Patient clinically improved with resolution of symptoms.Patient re-presented at 6 months, with 3 days of fever, irritability, emesis, and staring spells. Physical exam consistent with left-sided weakness and left upper extremity spasticity. Initial labs showed anemia 9.3 gm/dL, procalcitonin 8.79 mg/dL and CRP of 16.5 mg/dL. Vancomycin and ceftriaxone empirically started. CSF culture, meningitis/encephalitis panel, and 16sDNA negative. MRI demonstrated evolving signs of ischemia along the right MCA, a subdural collection with hemorrhagic contents and right cochleovestibular malformation involving the membranous labyrinth. Workup notable for low IgE, normal immunoglobulins and lymphocyte subsets. Genetic panel normal: (GDF15, amino acid, organic acid, carnitine, homocysteine, mito genome, hearing loss, brain malformation). CT demonstrated abnormalities in the internal auditory canal, incomplete partition of the membranous labyrinth to include abnormal cochlear with only 1.5 turns with no Modiolus or interscalar septum, dilated vestibule, enlarged semicircular canals and concerns of CSF communication with the right ear. Discharge on Augmentin for prophylactic treatment and referred to an outside hospital for right cochlear implantation.
Discussion: Recurrent meningitis (two or more episodes separated by complete resolution of symptoms) (1), secondary to congenital inner ear malformation is a rare clinical entity (2). Mondini is a developmental ear inner defect that leads to a short, flat cochlea and a less-than-expected number of turns (1 to 1.5 vs 2.5 to 2.75) (3). This abnormality causes communication between the subarachnoid space and the middle ear; leading to recurrent, retrograde meningitis (2). When the condition is suspected, CT of the brain is the gold standard for diagnosis, cochlear implants are necessary to correct the defect and prevent further episodes of meningitis (3).
Conclusions: Recurrent meningitis has a high mortality and fatal neurodevelopmental sequelae if left untreated. We present a 6 months old unvaccinated patient with Mondini dysplasia diagnosed in the setting of recurrent meningitis associated with unilateral sensorineural hearing loss. The condition could be an isolated finding or associated with gene loci mutations and congenital disorders. CT scan of the temporal bones should be obtained in patients with recurrent meningitis associated with hearing loss to facilitate early diagnosis. Cochlear implantation needs to be performed to prevent devastating neurological outcomes and recurrent meningitis