Background: In the inpatient setting, serum potassium (K) and magnesium (Mg) are frequently replaced for patients with values within the reference range (generally K 3.5-5.0 mEq/L, Mg 1.3-2.2 mEq/L) to target an arbitrary goal of 4 mEq/L for K and 2 mEq/L for Mg.(1,2) For certain high-risk non-pregnant adults, K and Mg replacement to these goals may be prudent. These high-risk groups include patients with heart failure receiving diuresis, recent myocardial infarction, arrhythmias, renal or gastrointestinal (GI) losses, and diabetic ketoacidosis or hyperosmolar hyperglycemic state.(3-6) However, for low-risk individuals there is no evidence to suggest that routine repletion of low-normal serum K and Mg levels (i.e. values within the normal reference range) carries any clinical benefit, such as reducing the incidence of tachyarrhythmias or improving mortality.(2,7-9) Moreover, unnecessary replacement of electrolytes in low-risk populations can lead to adverse effects, including GI upset, venous irritation, and hyperkalemia and hypermagnesemia, which are associated with increased risk of arrhythmias and mortality.(7,8,10) Overutilization of K and Mg replacement can also increase healthcare costs and burden patients, nurses, and prescribers.(2)
Purpose: Our objective was to create an electronic medical record (EMR)-based order set that incorporates a patient risk assessment tool to ultimately reduce unnecessary repletion of normal K and Mg values for low-risk patients.
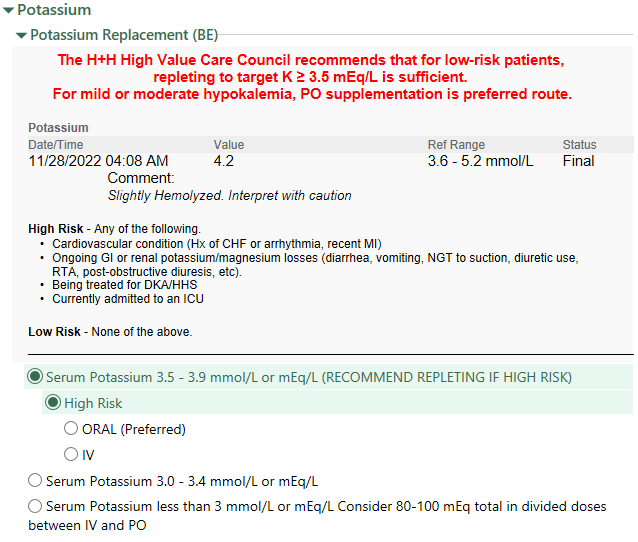
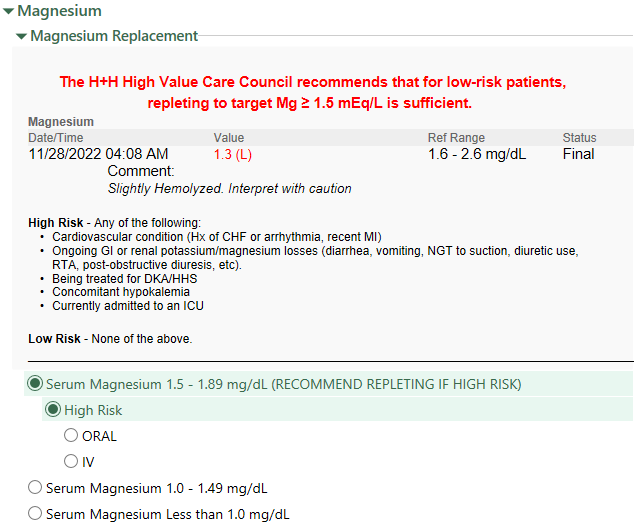
Description: The electrolyte replacement risk assessment order set was implemented on May 25, 2022. The order set provides information on which patients have high-risk predisposing conditions for morbidity related to electrolyte deficiency and recommends deferring repletion for low-risk patients with normal K and Mg levels. If the high-risk option is selected, the prescriber is prompted to order the appropriate replacement through the order set (Figures 1 and 2). Data regarding the average weekly replacement rate for K and Mg were collected. We compared data from the pre-intervention period (January 1, 2021 – May 24, 2022) to the post-intervention period (May 25, 2022 – November 26, 2022). The rate of electrolyte replacement decreased significantly after the implementation of the electrolyte replacement risk assessment order set for both K and Mg. Between the pre-intervention period and post-intervention period, the rate of K replacement decreased by 9.6% (from 106.5 to 96.3 repletions/1000 patient-days, p< 0.01). Between the pre-intervention period and post-intervention period, the rate of Mg replacement decreased by 23.5% (from 102.2 to 78.2 repletions/1000 patient-days, p< 0.01).
Conclusions: Implementation of an electrolyte replacement order set with an integrated patient risk assessment tool resulted in a reduction in K and Mg replacement ordered in our hospital system. Our findings suggest that a simple EMR-based tool targeting unnecessary repletion of normal K and Mg values in low-risk patients can decrease the overutilization of potassium and magnesium replacement.