Background: Hospital-acquired venous thromboembolism (VTE) is a common complication that leads to prolonged hospitalizations 1 and increased morbidity and mortality 2. Data analyzed from the Computerized Registry of Patients with VTE (RIETE) suggests that 1 in every 3-4 patients with VTE develop this condition in the hospital 3. A study done using data collected from the Canadian province of Quebec health care database demonstrated that of those patients who developed a hospital-acquired deep vein thrombosis (DVT), the 30-day and 1-year mortality rates were 10.6% and 23% respectively 4. Despite this increased risk, maintenance of VTE prophylaxis is typically ensured only by manual order checks, and rates of accurate documentation surrounding VTE prophylaxis is suboptimal, highlighting a need for additional quality assurance measures.
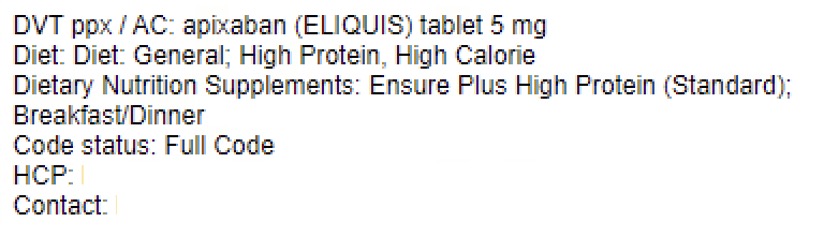
Methods: To address discrepancies between VTE prophylaxis orders and documentation in the electronic medical record (EMR), we developed a SmartText (Figure 1) within the EMR that used active orders to auto populate important information such as DVT prophylaxis, code status, diet order and health care proxy. We then created standardized progress note templates to be used across the inpatient medicine service at Bellevue Hospital and embedded the new SmartText into the progress note template. We reviewed usage of the SmartText as a surrogate measure of documentation accuracy regarding VTE prophylaxis for the 6 month period post-intervention. We also analyzed pre- and post-intervention frequencies of hospital-acquired VTE to determine if our intervention reduced the rate of hospital-acquired VTE.
Results: Prior to introducing our intervention, we reviewed charts of 50 patients admitted to inpatient medicine teams at Bellevue Hospital to determine pre-intervention documentation accuracy. Of the 50 charts reviewed, 68% correctly documented what was actually ordered for VTE prophylaxis. We reviewed the rate of SmartText usage for the 6 months after the intervention was introduced. Results showed that documentation accuracy had improved to 92%. We also reviewed the frequency of hospital-acquired VTE pre- and post-intervention. Prior to the intervention, the rate of hospital-acquired VTE on the medicine service was 0.311 events per 1000 patient days. After the intervention, the rate of hospital-acquired VTE on the medicine service was 0.225 events per 1000 patient days. This represents a 28% reduction in hospital-acquired VTE (p< 0.001).
Conclusions: Introducing standardized documentation with practical SmartTexts, is an easily implementable and highly impactful intervention to improve the accuracy of documentation surrounding VTE prophylaxis orders. In addition, implementation of this standardized documentation effectively reduced hospital-acquired VTE. Next steps include implementing this SmartText throughout the rest of our hospital system – NYC Health and Hospitals. In addition, we will also consider developing additional standardized documentation tools with a goal of reducing the incidences of other hospital-acquired conditions.