Background: Lab testing is critical for clinical decision-making and used throughout healthcare systems. Overuse of lab testing is known to be commonplace and contributes to shortages in lab testing materials. While practices exist at medical institutions that aim to limit lab test overuse, it is unclear which interventions are effective.
Methods: We aimed to reduce unnecessary inpatient serum magnesium laboratory testing through Lean methodology, which included (1) investigation of magnesium testing practices, (2) identifying root causes of low-value tests (3) designing and implementing an intervention plan that limited the number of recurrent, sequential magnesium lab tests that can be ordered, and (4) monthly tracking of changes to magnesium lab testing. We examined the historical volume of magnesium lab tests ordered and stratified them by service line. In addition, we surveyed front-line clinicians on their cognitive processes in ordering magnesium tests. Utilizing the quantitative and qualitative data, we performed a root cause analysis with Lean tools and identified largest, intervenable contributors to unnecessary magnesium lab tests. An intervention plan was designed and implemented hospital-wide, and we compared the number of magnesium lab tests ordered between the pre-intervention period (Apr-Spt 2021) and post-intervention period (Oct 2021-Apr 2022). We designed and implemented an electronic health record intervention that limited the computerized ordering of recurrent magnesium lab tests to a maximum of 4 instances within a 48 hour period, along with clinician education.
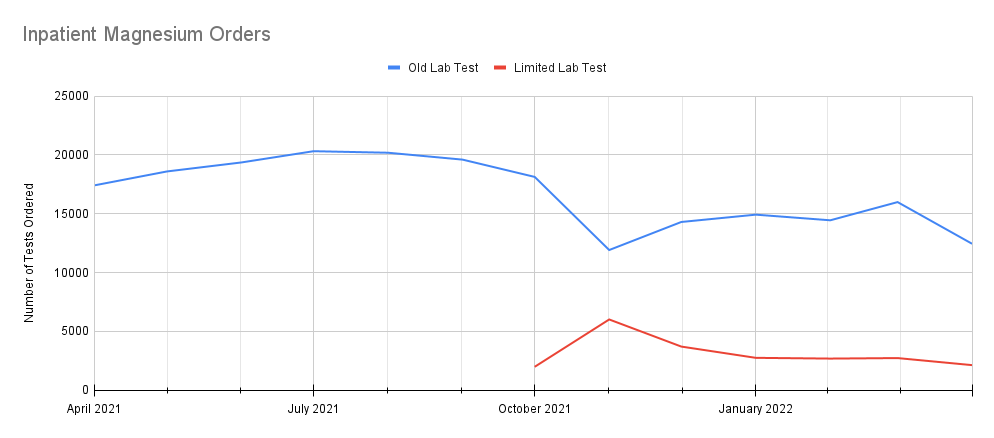
Results: Magnesium lab tests were found to account for approximately $1 million in direct costs over the course of a year with only 25% of those tests coming back as abnormal. The top 5 service lines ordering magnesium tests were identified to be Cardiac Surgery, Cardiology, Hospitalist, Hematology and BMT. At 6 months post-intervention, we found an 8% overall reduction in magnesium lab testing and a ~24% reduction in the original magnesium lab orders (Average Total: 19,244/month pre vs 17,725/month post; Average Original Lab Order: 19,244/month pre vs 12,811/month post) without significant changes in rapid responses/code blues. Savings thus far on the order of $70,000 – $80,000 extrapolated for the year.
Conclusions: Changes to order capabilities for magnesium testing are able to drive down overuse as well as result in hospital-wide savings. Limits on recurrent lab test orders in general may reduce overuse without impacting patient safety.