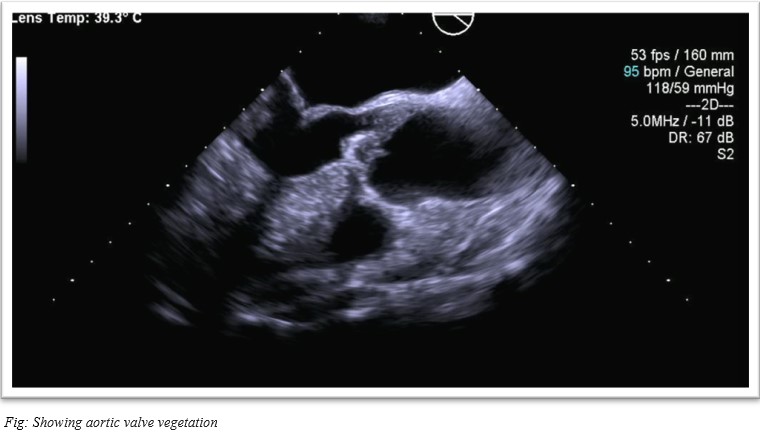
Case Presentation: Fifty-five year-old-male presented with worsening tremors associated with fever, and generalized myalgias. On examination was found to have a low-grade fever, supraventricular tachycardia with elevated troponins, and a tender left inguinal lymph node. On further examination with transthoracic echocardiogram he was found to have new moderate aortic insufficiency, with a thickened sclerotic aortic valve, followed by thickened echo density in the aortic valve concerning vegetations was seen in transesophageal echocardiogram. He had initially tested positive for Tropheryma whipplei (T. whipplei) on a polymerase chain reaction (PCR) test. He was started on doxycycline and hydroxychloroquine for twelve months with a repeat PCR test for Tropheryma whipplei every six months. The patient tested negative in four consecutive tests following the initiation of therapy and has been doing well for the past seven years on follow-up with no relapse.
Discussion: Whipple’s endocarditis is a rare disease, isolation of which is difficult and seldom reported in literature. This is partly because it is classified as blood culture-negative infective endocarditis and generally does not satisfy Duke’s criteria. Whipple’s disease is seen as arthralgia, weight loss, and malabsorption syndrome. T. whipplei endocarditis is an emerging invasive entity of Whipple’s disease affecting middle-aged men. 20% of those reported do not have associated Whipple’s disease. The most common heart manifestations are heart failure, valvular disease, and peripheral arterial embolism. It is confirmed by PCR amplification. Our patient presented with new arrhythmia, with low-grade fever, which is unusual. We could not get a biopsy from the valve, but the PCR amplification confirmed the diagnosis, earlier than usual. Based on the literature review, it takes 8 months on average, from the onset of arthralgia to diagnosis of endocarditis. We were able to diagnose and start therapy early, before the onset of arthralgia, and successfully treat the endocarditis without any complications which improved the patient’s quality of life. He is able to continue with his daily life as he was before the onset of endocarditis.
Conclusions: T. whipplei endocarditis is a rare disease, when diagnosed early with proper history taking and workup, an early start of treatment can preserve the quality of life in middle-aged patients, considering that these patients have high mortality and relapse rates.