Background: The 2011 AAP policy statement regarding recommendations for a safe infant sleeping environment included hospitalized infants, but unsafe sleep practices continue to be common in hospitalized infants. Safe sleep position compliance was observed to be low at Baystate Chidlren’s Hospital (BCH), as described in a prior abstract (http://abstract.staging.hospitalmedicine.org/abstract/improving-infant-safe-sleep-practices-in-the-inpatient-setting-using-qi-methodology/). Interventions designed to improve rates of safe sleep practice (SSP) and education during hospitalization have been described in the literatures, but few have incorporated family centered rounds (FCR) as part of the process. Our objective was to assess baseline rates of safe sleep reinforcement and education during FCR as part of ongoing QI efforts to improve safe sleep education and reinforcement.
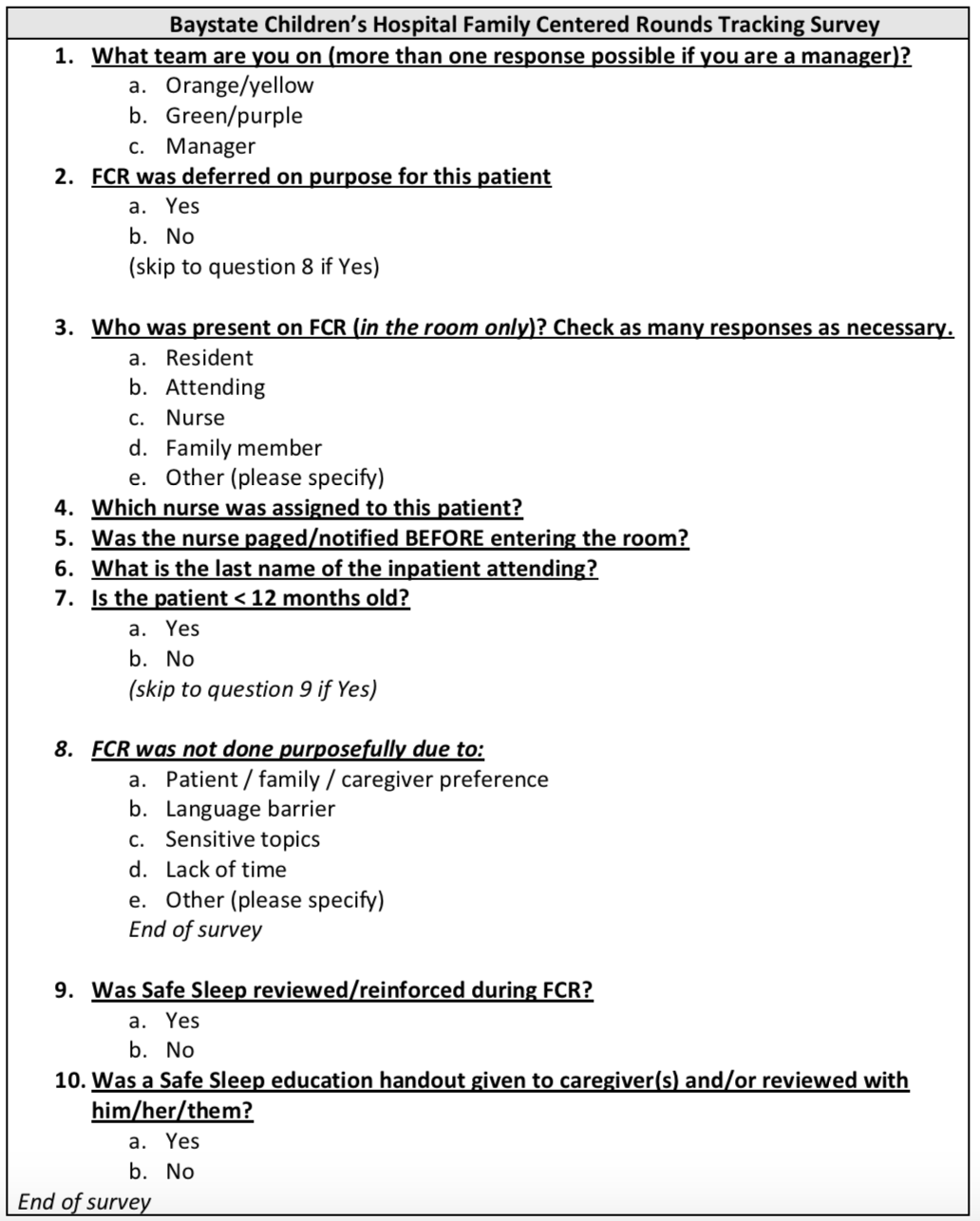
Methods: At Baystate Children’s Hospital (BCH), FCR is tracked through an electronic survey (www.surveymonkey.com, LLC; Palo Alto, CA) completed by resident physicians after each patient visit. Its development and implementation is described in a prior abstract (http://abstract.staging.hospitalmedicine.org/abstract/effect-of-teaching-team-structure-on-rates-of-nursing-and-family-attendance-during-family-centered-rounds/). Survey questions addressed team assignment, if FCR was deferred and why, who was present, and nurse/attending physician name (Figure 1). Since April 2018, if the patient was 12 months old, questions were added addressing whether safe sleep was reviewed and education provided to provide a baseline for further QI interventions. Data was reviewed from April 1 to November 30, 2018.
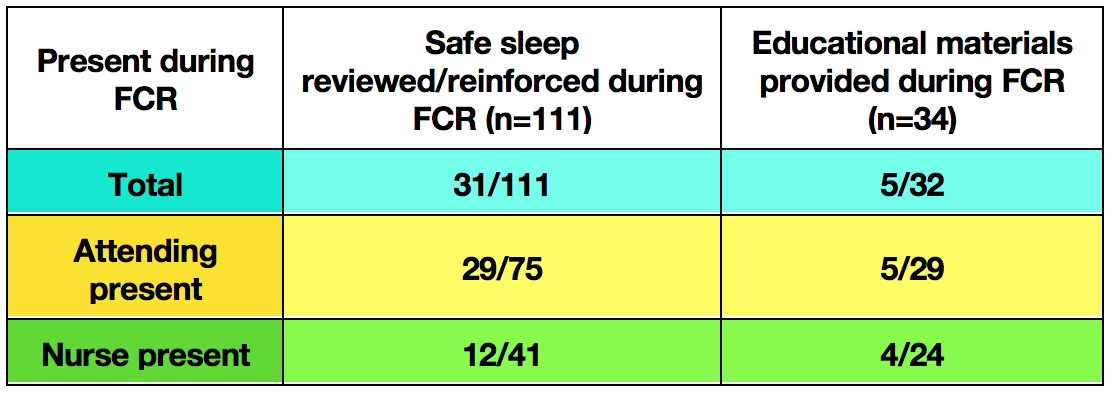
Results: Of 767 surveys were completed during this period, 113 surveys indicated the patient was 12 months old. Of these, Question 9 (“Was Safe Sleep reviewed/reinforced during FCR?”) was answered in 111 surveys and Question 10 (“Was a Safe Sleep educational handout given to caregiver(s) and reviewed with him/her/them?) was answered in 34 surveys. Based on survey responses, safe sleep was reviewed/reinforced during 28% of visits, and education handouts were given and reviewed during 14% of visits (Table 1). This did not vary significantly based on attending or nursing presence.
Conclusions: At our institution, rates of safe sleep reinforcement and education during FCR are low, and do not vary based on attending or nursing presence. Future interventions to address safe sleep during FCR and at other times during hospitalization may improve rates of observed safe sleep during hospitalizations.