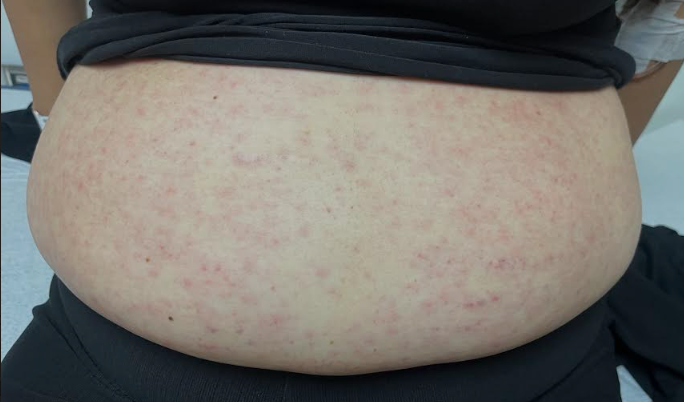
Case Presentation: Systemic lupus erythematosus (SLE) is an autoimmune disorder of unknown etiology that can involve virtually any organ system. This case highlights the diagnosis of lupus in a severely neutropenic patient, emphasizing the diverse manifestations and associations of the disease. A 39-year-old female presented to the emergency department with a persistent, diffuse maculopapular rash following amoxicillin treatment for streptococcal pharyngitis. Laboratory results were significant for absolute neutrophil count of zero, a protein gap, and anemia. The patient was admitted for evaluation of severe neutropenia. An exhaustive infectious work-up revealed recent Epstein Barr Virus (EBV) infection. The patient’s neutropenia persisted, and full body CT showed diffuse lymphadenopathy. A review of the clinical literature identified fewer than ten cases of neutropenia caused by EBV. Given the complexity of the presentation, the differential was broadened to include rheumatological etiologies as well as malignancy. Subsequent work-up included biopsies of the rash, bone marrow and lymph nodes as well as flow cytometry and peripheral smear. A diagnosis of systemic lupus erythematous (SLE) with was confirmed with positive ANA (1:2560, speckled pattern), elevated anti-DNA antibodies, low C4, and interpretation of tissue biopsies. Renal biopsy was subsequently performed and unexpectedly revealed IgA nephropathy. The patient’s acute lupus flare was treated with hydroxychloroquine and high dose steroids after which her neutropenia resolved.
Discussion: Cytopenias are a major hematologic consequence of systemic lupus erythematosus. Severe neutropenia with lupus can occur by a variety of mechanisms, including disease progression, development of anti-WBC antibodies and associated infection, either as the cause or consequence of neutropenia (1). In addition, serious infectious complications develop in up to fifty percent of patients with SLE. Thus, the patient’s initial rash and IgA nephropathy – potential post-infectious complications – could still reasonably be related to undiagnosed lupus.
Conclusions: Overall, the above findings support a diagnosis of secondary autoimmune neutropenia in the setting of acute lupus. This case illustrates the varied and sometimes unusual presentations of lupus, highlighting the importance of maintaining a broad differential diagnosis. It emphasizes the need for a thorough rheumatologic evaluation when other findings (i.e., coexisting infections) do not fully explain the clinical picture.