Background: In Texas, the five-year survival rate for lung cancer is significantly lower compared to the national average with noted disparities in early diagnosis and treatment. The aim of this study is to assess sex, ethnic and racial differences in end-of-life healthcare utilization, advance care planning (ACP) and associated outcomes such as hospice use among Texan Medicare lung cancer decedents.
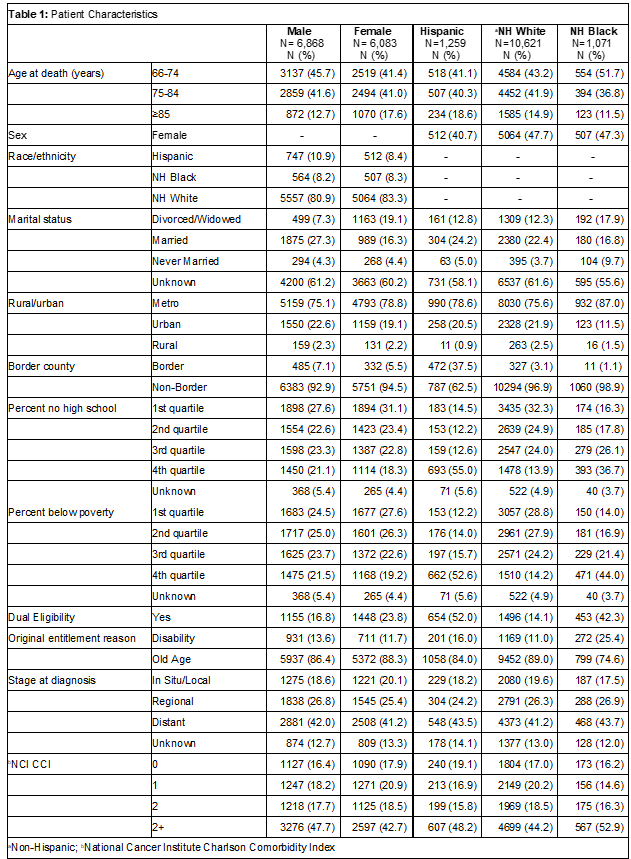
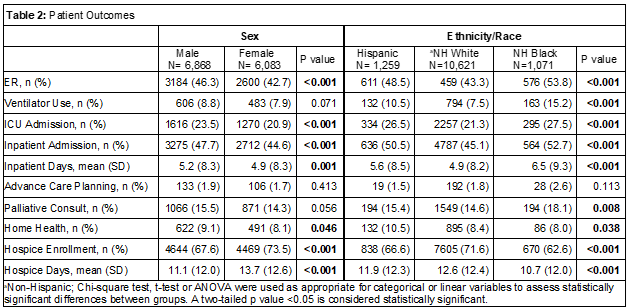
Methods: We analyzed Texas Cancer Registry linked with Medicare data for patients aged 66 years and older who died 6 months to 5 years after receiving a diagnosis of primary lung cancer from 2010-2018. Patient characteristics including age at death, original entitlement reason and stage at diagnosis are reported as frequency (proportion) or mean (standard deviation (SD)). Chi-square test, t-test or ANOVA were used as appropriate for categorical or linear variables to assess statistically significant differences in healthcare utilization, ACP and downstream outcomes between groups in the last 30 days of life. Multivariable logistic regression models were used to assess sex, ethnic and racial differences in odds of inpatient admission or hospice enrollment in the last 30 days of life.
Results: A total 12,951 decedents with 6,868 (53%) males and 6,083 (47%) females were included in analyses. Most (10,621 (82%)) patients were non-Hispanic White while 1,259 (10%) were Hispanic and 1,071 (8%) were non-Hispanic Black (Table 1). Significantly more males had an emergency department (ED) visit, intensive care unit (ICU) admission, inpatient admission and more inpatient days when compared to females in unadjusted analyses (Table 2). Males and females had low rates of ACP (< 2%). However, more females were hospice enrolled with more days in hospice compared to males. While multivariable logistic regression models did not show a significant difference in odds of inpatient admission, females had greater odds of hospice enrollment compared to males (odds ratio (OR) 1.28, 95% confidence interval (CI) 1.18-1.38). More non-Hispanic Black decedents, followed by Hispanic decedents, had ED visits, ventilator use, ICU admission, inpatient admission and more inpatient days in the last 30 days of life compared to non-Hispanic White decedents, respectively (Table 2). While ACP was low across all groups, there were no statistically significant differences. More non-Hispanic White decedents were hospice enrolled with more days in hospice compared to minoritized decedents. Multivariable logistic regression models showed that non-Hispanic Blacks had greater odds of inpatient admission (OR 1.39, 95% CI 1.21-1.60) and lower odds of hospice enrollment (OR 0.64, 95% CI 0.56-0.74) compared to non-Hispanic White decedents. Models also showed that Hispanics had more inpatient admissions (OR 1.38, 95% CI 1.19-1.59) and less hospice enrollment (OR 0.83, 95% CI 0.72-0.96) compared to non-Hispanic White decedents, respectively.
Conclusions: Among Texan Medicare lung cancer decedents, we found that males, non-Hispanic Black and Hispanic decedents had greater healthcare utilization and less use of hospice in the last 30 days of life. These differences could be due to a variety of factors including cultural preferences and availability and access to quality hospice and other services among others. ACP rates were low across all groups, possibly marking an important opportunity for providers to address patient priorities and assure provision of patient-centered care at the end-of-life.