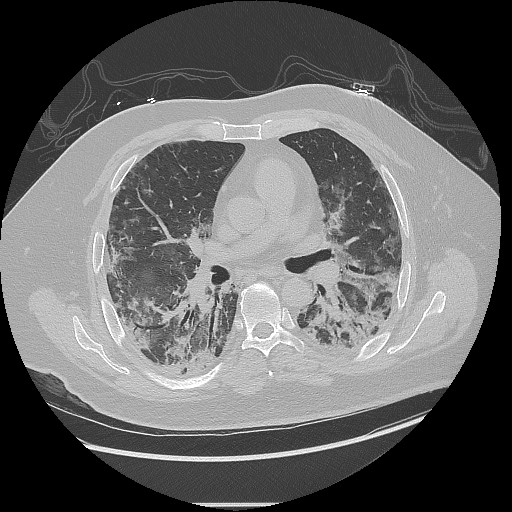
Case Presentation: A 44 year-old male with a history of gout presented with bilateral hand swelling, muscle weakness, fatigue, rash, and shortness of breath. The symptoms have progressed for the last 6 months to the point of inability to walk more than a block and needing assistance getting up despite a course of standard gout treatment. Over the last 2 weeks he has developed a new chest rash that did not improve with prescribed antibiotics. Vitals on arrival are notable for hypoxia to 84% requiring 10 liters of oxygen by nasal cannula but otherwise hemodynamically stable. Physical exam is notable for scattered crackles throughout his lung fields, an erythematous blanching maculopapular rash across the chest wall, and heliotrope-pattern rash. Computed Tomography (CT) of the chest reveals findings suggestive of interstitial lung disease (ILD) associated with mixed connective tissue disease in a non-specific interstitial pneumonia pattern. Initial labs revealed ferritin elevated at 4606 ng/mL, lymphopenia to 640 cells/uL, negative antinuclear antibody, antineutrophil cytoplasmic antibody, rheumatoid factor, and anti-cyclic citrullinated peptide. A myomarker panel was positive for anti-Melanoma differentiation-associated protein-5 (MDA5) antibody. He was diagnosed with anti-MDA5+ dermatomyositis (DM) with rapidly-progressive ILD and treated with high dose methyl-prednisolone, tacrolimus, and rituximab.One week into hospitalization, CT Abdomen and Pelvis was notable for a left retroperitoneal hematoma and diffuse intramuscular iliopsoas hemorrhage with layering effect suggestive of active bleeding. The patient developed hemorrhagic shock and unfortunately passed from multiorgan failure.
Discussion: Anti-MDA5+ DM is a subtype of DM characterized by a unique clinical spectrum that includes rapidly-progressive ILD, skin manifestations (ulcerations, alopecia, Gottron papules, heliotrope rash, or shawl rash), inflammatory arthropathies, and a lower incidence of muscle involvement compared to other forms of DM1. While there are no formal diagnostic criteria or treatment guidelines, serologic testing should be considered in those with rapidly-progressive ILD and notable skin findings. Treatment with a combination of high-dose glucocorticoid, cyclophosphamide, and calcineurin inhibitors has been shown to improve survival and pulmonary function compared to a step-up regimen2. Respiratory failure is the most common cause of death, but there has been emerging evidence of spontaneous intramuscular hemorrhage as a cause of mortality, with development of deep tissue hemorrhage associated with 50-60% mortality rate in retrospective analyses occurring in the first month after diagnosis2,3. Among patients with DM, risk factors for mortality include presence of ILD, elderly age, male gender, anti-MDA5 positivity, lymphopenia, hyperferritinemia, and elevated creatine kinase1. The first four of these factors have also been associated with development of spontaneous intramuscular hemorrhage, as well as high dose steroid use and heparin use, though the rarity of this complication makes it difficult to interpret clinical associations2.
Conclusions: This case highlights the clinical features of anti-MDA5+ DM, including skin findings, rapidly-progressive ILD, positive serologic testing, as well as a rare but severe complication of spontaneous intramuscular hemorrhage. Early identification of the disease and awareness of leading causes of mortality is prudent to help prolong survival.