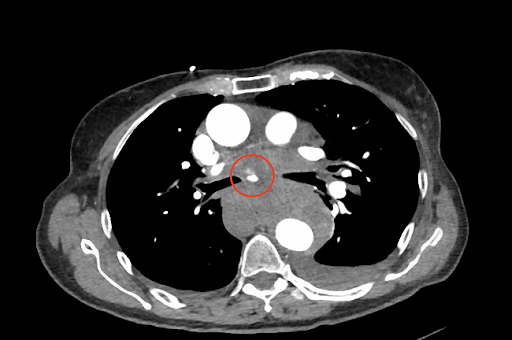
Case Presentation: An 80 year old female presented with severe interscapular back pain of abrupt onset with radiation to the epigastrium. There was no preceding trauma. 43 days prior to current presentation, she was hospitalized for acute pulmonary embolism and was discharged home on apixaban. Other past medical history included hypertension, hyperlipidemia and coronary artery disease. CT angiogram of chest with contrast revealed a bronchial artery pseudoaneurysm (BAP) and hemomediastinum. Anticoagulation was urgently reversed with prothrombin complex concentrate. A thoracic aortogram and selective bronchial artery angiography failed to localize the bleeding site, hence therapeutic bronchial artery embolization (BAE) was unsuccessful. Mid-procedure, she became hemodynamically unstable. Emergent exploratory thoracotomy was performed with evacuation of a large mediastinal hematoma. 3 hours later, high volume bloody chest tube output was observed necessitating repeat surgical exploration, blood transfusions and clotting factors. Mediastinal packing was performed and topical hemostasis was achieved. Following surgery, her hemodynamics were closely monitored in the ICU. Given recent history of thromboembolism, venous dopplers were obtained and revealed bilateral soleal DVTs. Anticoagulation was contraindicated. Once her condition stabilized, an IVC filter was placed and patient was discharged on day 10. Unfortunately, two days later she was rehospitalized with right flank pain and shortness of breath. CT chest with contrast demonstrated hemomediastinum, right hemothorax and a BAP more pronounced this admission. Repeat thoracic aortogram and selective bronchial angiography were able to visualize a hypertrophied bronchial artery along with a BAP actively extravasating into the mediastinum. A second attempt at embolization was successful in cessation of mediastinal hemorrhage. She was safely discharged and on outpatient follow up in 7 weeks, there were no further reports of recurrence.
Discussion: BAP is a rare entity of unknown etiology. Previously, it has been associated with inflammatory lung conditions and infections such as bronchiectasis and pulmonary tuberculosis , trauma, and AV malformations. Our patient lacked related history suggesting spontaneous rupture. There is limited literature discussing spontaneous BAP rupture amidst anticoagulant therapy. Initial imaging usually comprises of a CT angiogram with contrast to detect hemomediastinum, a thoracic aortogram to localize the bronchial artery of interest and a selective bronchial artery angiography for enhanced visualization. < 1% of patients are ultimately diagnosed as it is often asymptomatic. Once rupture occurs, however, lethal complications can develop. Thus, corrective interventions should be pursued if incidentally discovered. Nonsurgical management with BAE is preferred in hemodynamically stable patients. It is less invasive than open thoracotomy which has a higher risk of mortality and is generally reserved for when BAE has failed or is contraindicated as in our patient with cardiovascular collapse during initial hospitalization.
Conclusions: This case illustrates challenges posed by a ruptured BAP. If unrecognized, life threatening hemorrhage can occur especially with concurrent anticoagulant use. Early detection is crucial for rapid diagnostic and therapeutic intervention. Unless contraindicated, transcatheter embolization is the treatment of choice.