Background:
Hospital discharge is a high risk transition for patients during which deficits in transfer of information between hospital providers and the primary care providers (PCPs) are common and lead to adverse events following discharge.
Purpose:
Consistent communication between hospital providers and PCPs at discharge may improve patient care.
Description:
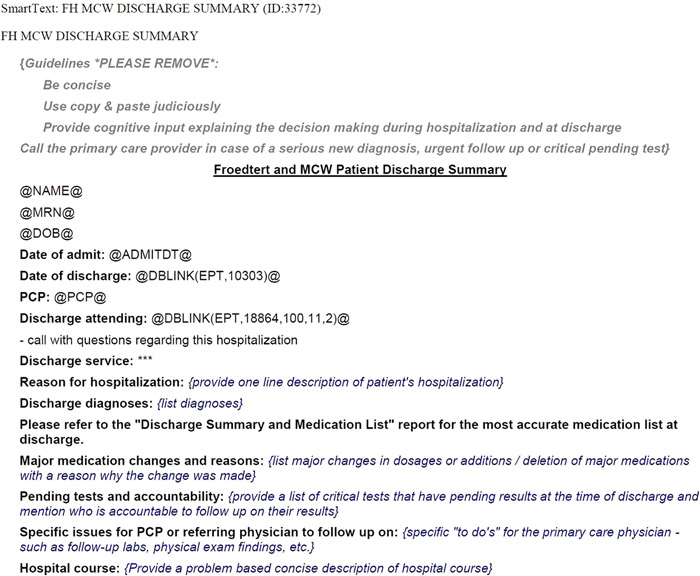
Our hospital is a 500 bed tertiary care academic medical center (AMC), with all specialties represented and utilizes a fully functional electronic health record (EHR). We first surveyed PCPs to get their perspectives about communication at discharge. PCPs preferred a high quality discharge summary as the ideal way to communicate with them upon most discharges. PCPs wanted concise information and elements such as pending tests, reasons for medication changes and instructions for outpatient continuation of care‐plan included in the discharge summary. They also rated the quality of discharge summaries from our hospital on a 1‐10 scale (10=excellent). We then analyzed the existing 18 different discharge summary templates in our EHR and found substantial variability. Inpatient providers initially claimed the need to have specialty specific discharge summary templates but upon participating in facilitated brainstorming sessions with each other, reached a consensus on a single discharge summary template (SDST) to be deployed across all specialties. The SDST met regulatory requirements; incorporated elements requested by PCPs and included ‘just in time’ reminders to help guide providers populating the template (in italics in Figure). Pharmacists helped create an accurate discharge medication list which was electronically appended to the SDST and gave a single secretarial person on every nursing unit (Health Unit Coordinator) the responsibility of reliably transmitting the SDST to the PCP. We deployed the SDST across all specialties in July 2013. A post‐deployment survey of PCPs in August 2013 found their rating of quality of discharge summaries from our hospital improved from 4.81 to 5.85 (p = 0.022).
Conclusions:
A standardized discharge summary can be deployed across all specialties in an AMC. Preliminary evaluation shows it improves PCP perception of quality of discharge summaries. Its impact on patient outcomes, including readmissions is ongoing.
Figure: A partial screen shot of the Standardized Discharge Summary.
PCP rating of quality of discharge summaries before and after deployment of the standardized discharge summary. PA = physician assistant
| Discharging Service | Pre‐Intervention | Post‐intervention | P‐Value (Mann‐Whitney) | ||||
| N | Mean | Median | N | Mean | Median | ||
| All specialties | 36 | 4.81 | 5 | 34 | 5.85 | 5.5 | 0.022 |
| Cardiology | 33 | 4.97 | 5 | 28 | 5.82 | 6 | 0.117 |
| Cardiothoracic Surgery | 27 | 4.56 | 5 | 22 | 5.41 | 5 | 0.216 |
| General Medicine — Overall | 36 | 5.89 | 5.5 | 33 | 6.67 | 7 | 0.110 |
| General Medicine — PA‐based Teams | 34 | 6.00 | 6 | 31 | 6.74 | 7 | 0.130 |
| General Medicine — Resident‐based Teams | 34 | 5.59 | 5 | 31 | 6.74 | 7 | 0.032 |
| General Surgery | 31 | 4.32 | 5 | 27 | 5.33 | 5 | 0.055 |
| Gynecology | 23 | 4.04 | 4 | 26 | 5.38 | 5 | 0.044 |
| Medical Oncology | 27 | 4.19 | 4 | 25 | 5.76 | 5 | 0.011 |
| Neurology | 30 | 3.93 | 4 | 27 | 5.63 | 5 | 0.004 |
| Neurosurgery | 22 | 3.82 | 4 | 24 | 4.96 | 5 | 0.048 |
| Orthopedics | 32 | 3.75 | 3.5 | 27 | 4.78 | 5 | 0.093 |
| Otolaryngology | 19 | 4.53 | 5 | 21 | 5.14 | 5 | 0.216 |
| Physical Medicine and Rehab | 23 | 4.87 | 5 | 21 | 5.48 | 5 | 0.314 |
| Plastic Surgery | 21 | 4.24 | 4 | 19 | 4.58 | 5 | 0.270 |
| Surgical Oncology | 22 | 4.86 | 5 | 20 | 4.60 | 5 | 0.718 |
| Transplant | 23 | 5.03 | 5 | 21 | 4.62 | 5 | 0.574 |
| Trauma | 23 | 4.57 | 5 | 22 | 4.41 | 5 | 0.799 |
| Urology | 23 | 4.91 | 5 | 21 | 4.76 | 5 | 0.895 |
| Vascular Surgery | 20 | 4.80 | 5 | 20 | 4.80 | 5 | 0.761 |