Case Presentation: Statin-induced necrotizing autoimmune myopathy (SINAM) is an immune mediated myopathy characterized by proximal muscle weakness and necrosis in the presence of autoantibodies to hydroxyl-methyl-glutaryl-coenzyme-A (HMG-CoA) reductase. It is a rare side effect of statin use that must be recognized quickly in order to prevent the development of irreversible muscle weakness. Most cases occur within the first year of statin use, although some may present sub-acutely with progression of symptoms following withdrawal of therapy. We report a rare case of an individual who developed SINAM two years after cessation of therapy.
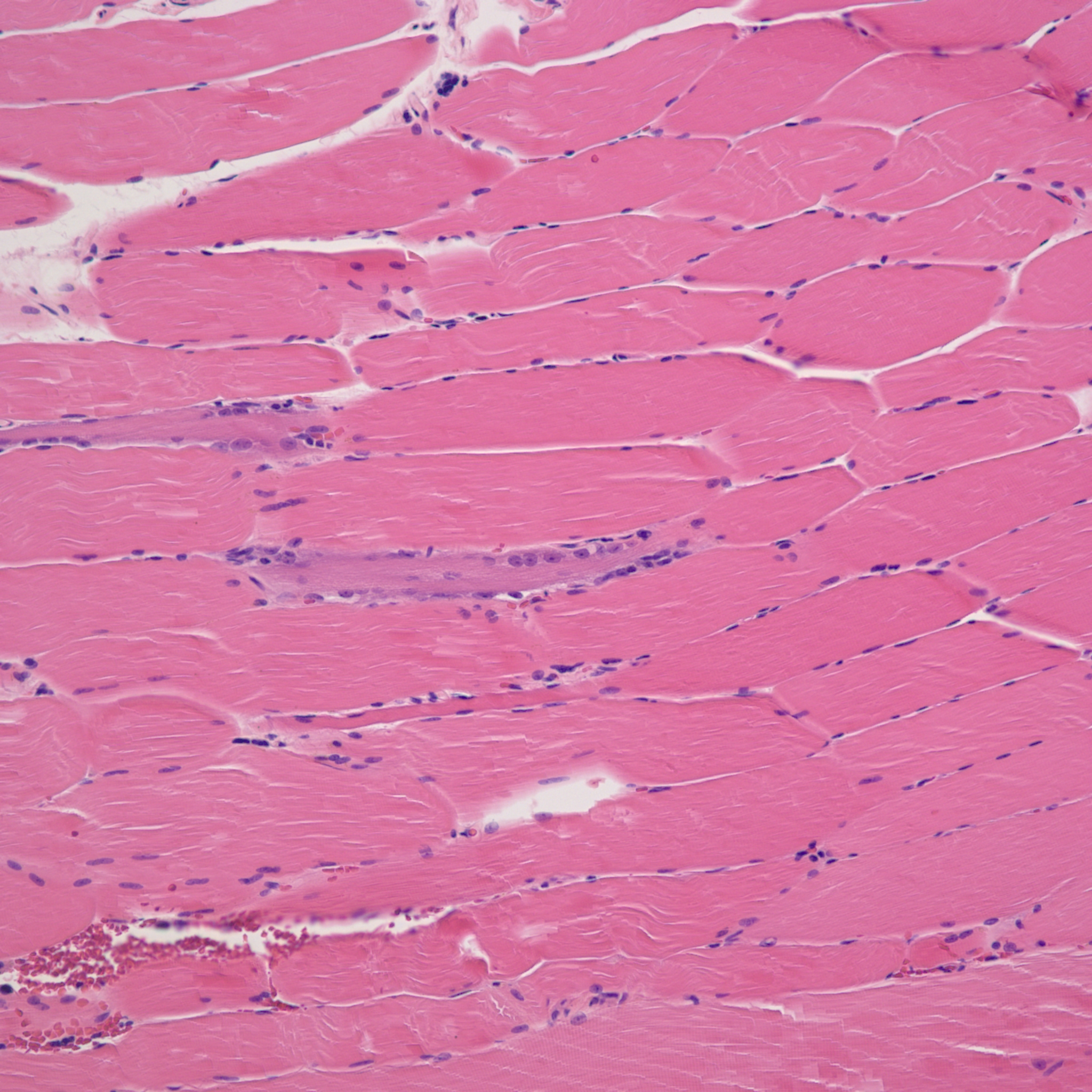
A 60-year-old Hispanic man with history of hypertension, hyperlipidemia, and hypothyroidism presented with several months of progressive myalgias and proximal muscle weakness. He had a history of atorvastatin use, but had discontinued it two years prior due to financial difficulties. Physical examination was notable for tenderness of the bilateral proximal lower extremity muscle groups as well as bilateral proximal upper and lower extremity muscle weakness. Initial laboratory evaluation was remarkable for a creatine kinase (CK) of 10,737, erythrocyte sedimentation rate (ESR) of 54, and C-reactive protein (CRP) of 11.30. Despite fluid resuscitation, muscle weakness and CK elevation persisted. Electromyogram (EMG) was concerning for muscle fiber necrosis; quadriceps muscle biopsy ultimately confirmed myopathic changes with necrosis. Subsequently, enzyme-linked immunosorbent assay (ELISA) revealed antibodies to HMG-CoA reductase, which, in concert with his clinical presentation and an extensive evaluation for alternate myopathic processes, suggested SINAM as the cause of his weakness. Pulse dose steroids and intravenous immune globulin (IVIG) were initiated with profound improvement in his weakness, after which he was transitioned to rituximab for continued immunosuppression.
Discussion: SINAM is an immune mediated myopathy manifested by muscle weakness in the setting of statin exposure. In contrast to other forms of statin-associated myotoxicity, including myalgias, myopathies, and rhabdomyolysis, SINAM is mediated by an autoimmune response and is associated with persistent or progressive symptoms despite statin discontinuation. SINAM generally occurs in the absence of risk factors for other statin-associated myotoxicities, but a genetic predisposition in individuals with certain HLA alleles has been described. Characteristic biochemical, EMG, and histologic findings support the diagnosis. Importantly, the irreversible muscle weakness seen in SINAM can be prevented with cessation of the offending agent and initiation of immunosuppression, so early and accurate diagnosis is critical to good clinical outcomes.
Conclusions: This case is unusual in that onset of myopathy occurred in a delayed fashion, although, with the increasing availability of ELISA testing for HMG-CoA reductase autoantibodies, it is felt that recognition of late onset SINAM may increase.