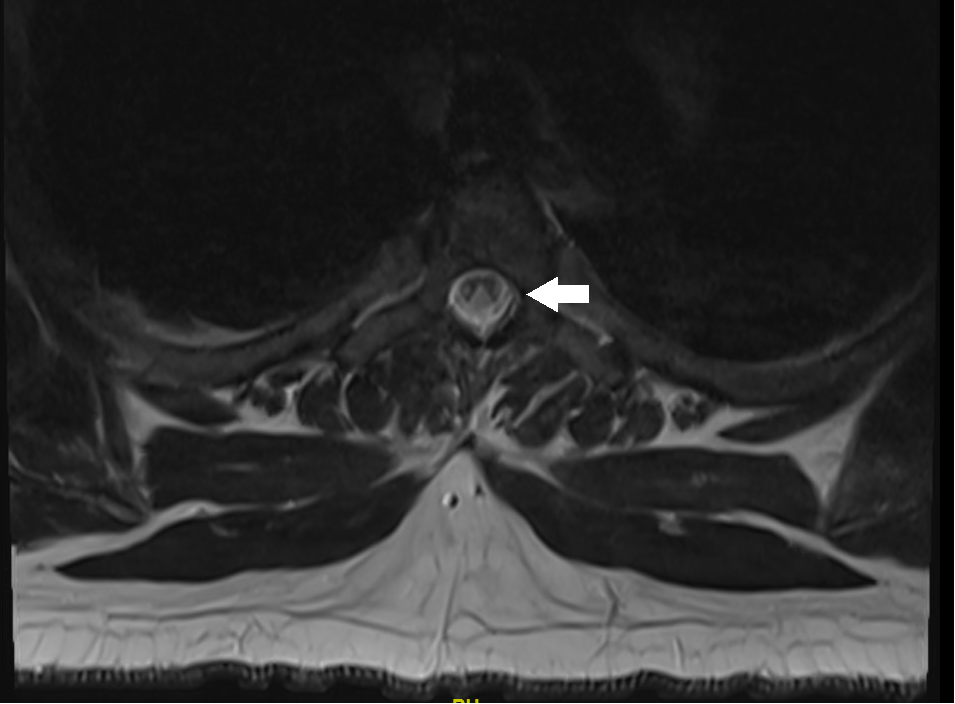
Case Presentation: A 32-year-old man with a remote history of alcohol and cocaine use disorders, depression and morbid obesity presented to hospital with numbness in the upper and lower extremities occurring over several months. His symptoms began with numbness and paresthesias in the hands and feet which was intermittent but became constant and spread proximally to involve the trunk at the mid-chest level. He described several falls due to unsteadiness and difficulty with ambulation. He denied neck pain, back pain, fever and chills, trauma, urinary or bowel incontinence.He was not taking medications at home. His occupation was gasoline pump repair technician. He reported daily cannabinoid and tobacco use, occasional alcohol use and initially denied other substances. On physical examination his vital signs were within normal limits. He was generally in no distress and morbid obesity was noted. Cardiac, abdominal, extremity and skin examinations were unremarkable. Neurological examination revealed normal mental status, fluent speech and intact cranial nerves. Sensory perception was severely diminished in a stocking-and-glove distribution to temperature, vibration and proprioception. Reflexes were 1+ biceps and triceps, 0 at brachioradialis, 3+ at the knees, and 0 at the ankles. Toes were upgoing bilaterally. His gait was wide-based and unsteady. Romberg sign was present. Muscle strength was normal throughout.Cerebrospinal fluid analysis revealed protein 50 mg/dL (reference 15-45 mg/dL), 1 nucleated cell and normal glucose. Magnetic resonance imaging (MRI) of the spine revealed diffusely abnormal signal intensity throughout the cervical and thoracic spinal cord predominantly involving the dorsal columns and to lesser extent the lateral cortical spinal tracts (Figure). Vitamin B12 serum level was 193 pg/ml (reference 211 – 911 pg/ml).Subacute combined degeneration due to vitamin B12 deficiency was strongly suspected. Upon further questioning the patient disclosed heavy use of “whippets,” or inhaled nitrous oxide. Parenteral cyanocobalamin (vitamin B12) supplementation was initiated, the patient was counseled to discontinue inhaled nitrous oxide use and referred for outpatient physical therapy.
Discussion: Nitrous oxide is a faintly sweet smelling gas inhaled recreationally for its empathogenic effects. It is easily available in small canisters known as “whippets” due to their intended use in homemade whipped cream preparation. Nitrous oxide misuse may lead to subacute combined degeneration (SCD) of the spinal cord through inactivation of vitamin B12. Chronic nitrous oxide ingestion leads to oxidation of vitamin B12 making it unavailable for myelin synthesis resulting in decreased myelination of the of the lateral and posterior columns of the spinal cord or SCD. Presenting symptoms include unsteadiness, paresthesias, and weakness. Examination findings include joint position and vibration sense loss, and sensory ataxia. Spinal cord MRI findings include dorsal T2 hyperintensity commonly in the cervical and thoracic regions. Treatment includes parenteral vitamin B12 supplementation and cessation of nitrous oxide use. Functional recovery is variable as a significant number of patients reported persistent paresthesias and sensory ataxia at follow up.
Conclusions: Chronic nitrous oxide misuse may lead to a functional B12 deficiency and present as a myeloneuropathy with signs and symptoms subacute combined degeneration of the spinal cord.