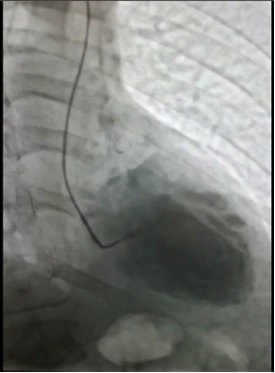
Case Presentation: Stress cardiomyopathy, also known as takutsubo cardiomyopathy, is a syndrome that causes transient cardiac apical akinesis or hypokinesis with concurrent basal hyperkinesis. This phenomenon occurs in the absence of angiographic evidence of obstructive coronary artery disease, often induced by emotional stress, and usually reverses within a few weeks to months. A rare variant is reverse takutsubo cardiomyopathy that can be triggered by various stressors. Basal ballooning occurs instead of the apical region and hypokinesis of the base with sparing of the mid-ventricle and/or apex.A 68-year-old male with past medical history of dementia, chronic alcohol use, seizure disorder, and adrenal insufficiency presented to the hospital with generalized weakness, chills, and poor oral intake for 3 days and 20-pound unintentional weight loss over the past few months. He was encephalopathic and hypotensive at 91/60. CT abdomen/pelvis and head showed no acute abnormalities except for hydropic gallbladder. With the patient’s history of adrenal insufficiency and daily fludrocortisone at home, he was given a loading dose of 100 mg hydrocortisone and started on norepinephrine drip in addition to simultaneous IV fluid boluses. However, he continued to be hypotensive and bradycardic for the following 12 hours. Troponin trended up to 2.75 ng/mL. Cardiology assessed for possible cardiogenic shock versus ischemic etiology. Continuous dopamine drip was added while attempts were made to wean norepinephrine. Cardiac catheterization revealed mild CAD. The left ventriculogram revealed dilated left ventricle, akinesis of the basal portion of the heart, and hypercontractile apex. Echocardiogram indicated left ventricular ejection fraction 35-40% with poor endocardial definition but mild to moderate global hypokinesis of the left ventricle.
Discussion: This case of reverse Takutsubo cardiomyopathy generally occurs in 2% of patients with stress-induced cardiomyopathy. It is hypothesized to occur as a result of catecholamine-induced vascular spasm of coronary arteries following extreme physical or emotional stress. This presentation was likely precipitated by the severe weight loss, anorexia, and poor oral intake with a possible component of acute adrenal insufficiency.Reverse takutsubo may not entirely follow the current theory of stress-induced cardiomyopathy since this case demonstrates hypokinesis of the basal portion of the heart while we see hypercontractility of the apex. This phenomenon may suggest the etiology to be related to myocardial receptor density, where a higher concentration of catecholamine receptors are present in the base compared to the apex embryologically.
Conclusions: Reverse Takutsubo cardiomyopathy is a rare occurrence that can be triggered by various stressors including cachexia and possible adrenal insufficiency as seen in this patient. Transient basal ballooning occurs with sparing of the apex, which occurs in the presence of minimal coronary findings. Left ventriculogram often demonstrates these cardiac wall motions well. The pathophysiology behind this disease is not well understood but could be either related to coronary vasospasms induced by catecholamine surges or by the density of catecholamine receptors in various regions of the cardiac muscles.